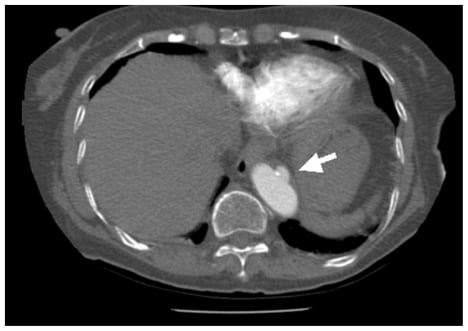
In emergency, ultrasound has been widely used as a noninvasive and effective examination to evaluate congestive heart failure. We highlight “Playboy Bunny” sign as a reliable marker and an important clue to the diagnosis of passive hepatic congestion, caused by congestive heart failure.
A 4-year-old boy underwent a tonsillectomy and adenoidectomy for tonsillar and adenoidal hypertrophy. The patient developed difficulty breathing after a nonbloody emesis during the car ride home after surgery.
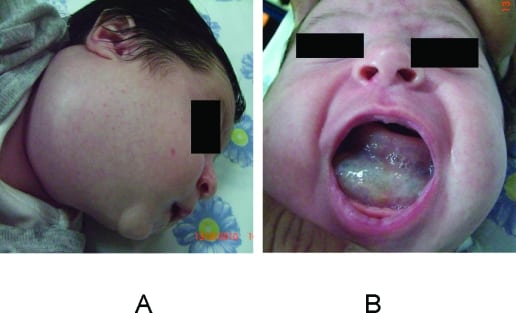
We report on a 3-month-old infant, who arrived in the pediatric emergency department (ED) with a cervical cystic hygroma causing an impending compromise of the airway. We recognize that such a lesion can rapidly progress, and the judicious use of imaging in the ED may help to avoid airway compromise and possibly fatal complications.
A 78-year-old male with multiple previous abdominal operations presented to the emergency department (ED) with abdominal pain and vomiting. Computed tomography (CT) revealed a small bowel obstruction.
We present the case of a 31-year-old trauma patient with computed tomography concerning significant C3–C4 subluxation. The abnormality is due to an artifact with which emergency physicians should be aware.
An 18-hour-old neonate was found to have absent movement of the left arm and a mildly edematous elbow following precipitous delivery with observed traction applied to the left arm.
A previously healthy 46-year-old male presented to the emergency department with the sole complaint of lower back pain after being struck by a car while walking. Physical examination revealed the patient to be hemodynamicaly stable and in moderate distress secondary to back pain.
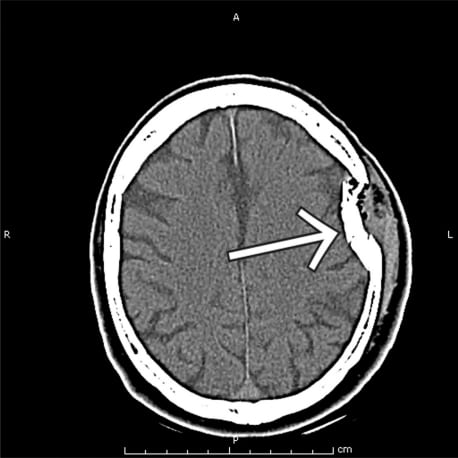
A 59-year-old male presented to the emergency department after having been struck on the head multiple times with a hammer. On presentation, vital signs were all within normal limits and primary exam was only impressive for a large left sided parietal-temporal hematoma.
A 51-year-old female with a history of gout, hypertension and diabetes presented to the emergency department with one week of increasing pain and swelling of her left knee, just below the patella. She denied trauma, fever and calf pain.
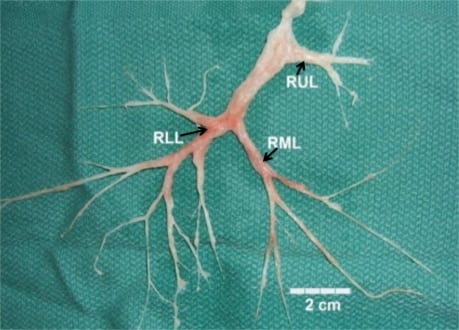
A 45-year-old male with a one-month history of dyspnea and cough presented with productive sputum consisting of bronchial casts for several days prior to admission.
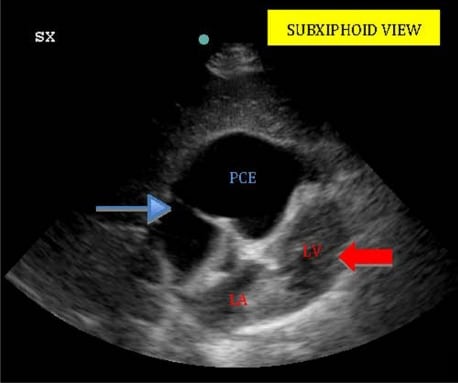
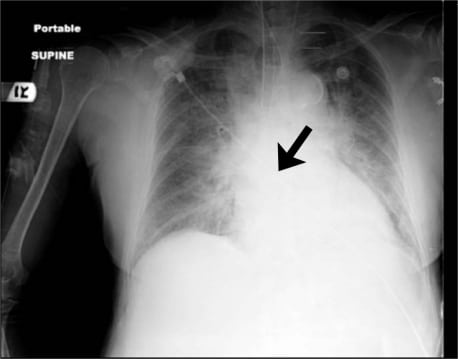
A 61-year-old man presented to the emergency department (ED) with gradual onset shortness of breath exacerbated by lying flat three weeks after undergoing minimally invasive three-vessel coronary artery bypass grafting (CABG).
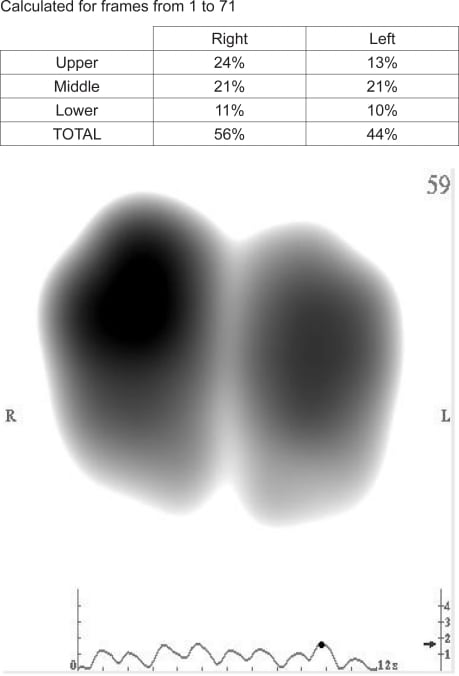
We are investigating the potential role for vibration response imaging (VRI) in the prompt emergency department (ED) evaluation of patients presenting with dyspnea to aid in differentiation between chronic obstructive pulmonary disease (COPD) and heart failure (HF).
This report highlights the importance of using bedside ultrasound in the emergency department to confirm guide-wire placement when performing central venous catheter placement prior to dilating and cannulating the vessel.
An adult male presented to the emergency department complaining of two days of exertional shortness of breath and progressive chest pain. He was afebrile with a blood pressure of 135/88 mmHg, heart rate of 105 beats/minute, respiratory rate of 22 breaths/minute, and a SaO2 of 94% on room air.
Ultrasound images of a patient presenting to the emergency department with expressive aphasia who was found to have carotid dissection. The first image is a standard two dimensional image that depicts the internal carotid with a visible flap within the lumen. The second image is a color Doppler image showing turbulent flow within the true lumen and visible flow within the false lumen. The case and the patient’s outcome are summarized along with some teaching points about carotid dissection. Also, there is some background and research on using ultrasound to help identify dissection.
A 79-year-old female presented to the emergency department complaining of two weeks of dyspnea on exertion and heart palpitations. A computed tomography (CT) pulmonary angiogram was obtained to rule out pulmonary embolism, which was negative.
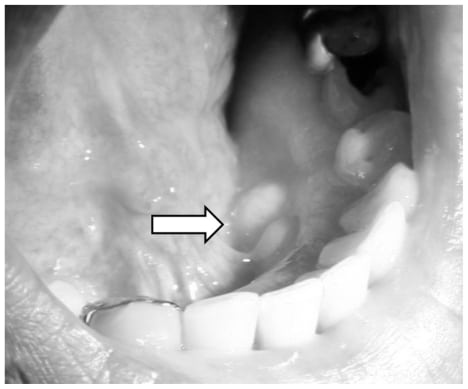
A 61-year-old man with a history of diabetes, hypertension, hyperlipidemia and polysubstance abuse presented to the emergency department complaining of bony growths on his lower jaw. He had noticed these growths intermittently in the past. He reported pain only when his dentures were in place and food lodged against the growths.
A 38-year-old woman with insulin-dependent diabetes reported four-days of flank pain, dysuria, polyuria and urinary urgency. Vital signs included blood pressure 113/70mmHg, heart rate 135/min, respiratory rate 24/min, and temperature 102.5°F. Exam revealed right cerebral vascular accident and suprapubic tenderness without guarding or rebound.
A 59-year-old female with a history of diabetes mellitus presented to the emergency department complaining of three weeks of an enlarging pulsating mass to her left buttock. The patient denied any associated trauma, leg pain, back pain or previous episodes. Physical exam was remarkable for a bounding non-tender pulsatile mass over the lateral left buttock.
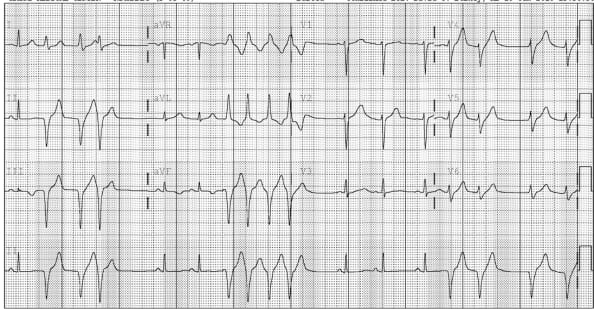
A 44-year-old Hispanic male with a history of Wolff-Parkinson-White Syndrome (WPW) presented with chest pain and palpitations that had been constant for three hours.
A 47-year-old woman presented with a history of an accidental fall against a glass door at home, causing a 15 cm-wide wound on the right gluteal region and hematuria. General health was good: blood pressure 115/70 mmHg with a heart rate of 100 beats/min; red cell count 4.460 x103/100 mL; hemoglobin concentration 10 g/100 ml; and hematocrit 31%.
Volvulus is a frequent condition in patients presenting in the emergency department (ED) with abdominal pain. While cecal volvulus occurs more often in young patients, sigmoid volvulus is more common in elderly patients.
A seven-year-old male presented with fever, left-sided facial redness, swelling and proptosis over a 24-hour period. He had noted left-sided toothache and rhinorrhea over the preceding week. On presentation, he stated that he was unable to see “anything, including light” from his left eye.
A previously healthy 38-year-old woman, with no significant past medical history, presented to the emergency department with acute onset of weakness after outpatient sclerotherapy. She had two milliliters of 0.5% foamed tetradecylsulfate injected into right lower extremity varicose veins. Twenty minutes after completion of the procedure, she had acute onset of right upper and lower extremity weakness.
A 22-year-old man presented to a rural Ugandan clinic with three months of progressive dyspnea. He described a non-productive cough and subjective fevers and chills. He appears mildly dyspneic but is in no acute distress.
A healthy 26 year-old G3P2 12 weeks pregnant with twins presented to the emergency department after the abrupt onset of palpitations, dizziness, shortness of breath and chest pain. An initial electrocardiogram demonstrated frequent preventricular contractions, which progressed to runs of sustained ventricular tachycardia (VT)
{kind=link}