
{kind=link}
| Author | Affiliation |
|---|---|
| Joshua R. Simmons, MD | Madigan Army Medical Center, Tacoma, WA |
| Brooks T. Laselle, MD | Madigan Army Medical Center, Tacoma, WA |
| David A. Della-Giustina, MD | Madigan Army Medical Center, Tacoma, WA |
ABSTRACT
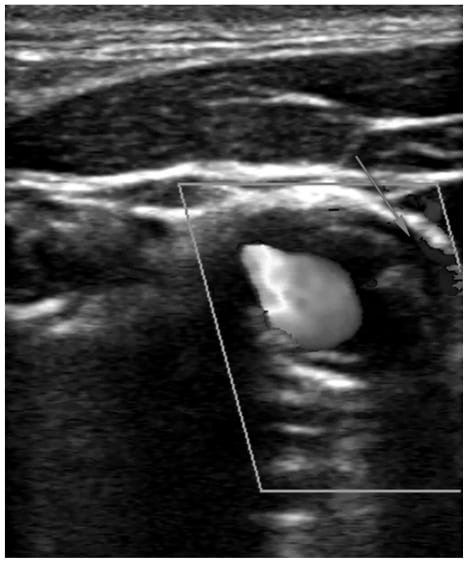
Ultrasound images of a patient presenting to the emergency department with expressive aphasia who was found to have carotid dissection. The first image is a standard two dimensional image that depicts the internal carotid with a visible flap within the lumen. The second image is a color Doppler image showing turbulent flow within the true lumen and visible flow within the false lumen. The case and the patient’s outcome are summarized along with some teaching points about carotid dissection. Also, there is some background and research on using ultrasound to help identify dissection.
CASE REPORT
A 78-year-old man presented to the emergency department (ED) with a five-minute episode of acute weakness, disequilibrium and dizziness that resolved without intervention. He had a negative evaluation, including head computed tomography (CT), magnetic resonance imaging and consultations by neurology and cardiology. He was discharged the next morning with a Holter monitor but represented several hours following discharge with a new expressive aphasia. Bedside ultrasound and CT angiogram at representation revealed carotid dissection with near complete occlusion. The patient underwent emergent stent placement of the left common and internal carotid arteries.
![Figure 1. Ultrasound of the common carotid artery showing an intimal flap (IJ) [arrow].](http://westjem.com/wp-content/uploads/2013/01/115-530-f.jpg)
DISCUSSION
Classically, carotid dissection should be considered in patients who present with symptoms of a transient ischemic attack or cerebrovascular accident who are younger than 45 or have a history of neck trauma. However, dissection may occur in older populations, those without antecedent trauma and in patients of any age with connective tissue disorders. Delay in diagnosis of carotid dissection is common because dissection usually presents with headache or neck pain prior to the development of neurologic symptoms, and since tests routinely ordered to evaluate neurologic complaints (i.e. noncontrast head CT or lumbar puncture) can fail to identify dissection.1,2 Standard two dimensional ultrasound can identify up to 72% of dissections and an additional 10% can be identified with use of color Doppler, which helps to highlight a false or double lumen. Combined with Doppler velocimetry, which is beyond the scope of the focused bedside evaluation for the emergency physician, the sensitivity is in the mid-90s.3
While Doppler techniques may require specialized training, they are not beyond the scope of emergency ultrasound. For carotid dissection ultrasound is very specific, but additional imaging should be obtained if the ultrasound is negative and dissection is suspected.3–5 In the ED, carotid ultrasound may allow rapid diagnosis of dissection leading to expedited and definitive care, such as the stent in this patient and avoiding potentially harmful, time-sensitive treatments, such as thrombolysis. Future studies should evaluate the feasibility of bedside carotid ultrasound by emergency physicians.
Footnotes
The views expressed are those of the author(s) and do not reflect the official policy of the Department of the Army, the Department of Defense or the U.S. Government.
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted May 20, 2010; Accepted July 16, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Joshua Simmons, MD, Intern, Emergency Medicine, Madigan Army Medical Center, 9040A Fitzsimmons Dr., Tacoma, WA 98431
Email: Joshua.R.Simmons@us.army.mil
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Stahmer SA, Raps EC. Carotid and vertebral dissections. Emerg Med Clin North Am. 1997;15:677.[PubMed]
2. Marx JA, Hockberger R, Walls R. Rosen’s Emergency Medicine. 7th edition. Mosby; 2010.
3. De Bray JM, Lhoste P, Dubas F, et al. Ultrasonic features of extracranial carotid dissections: 47 cases studied by angiography. J Ultrasound Med. 1994;13:659–64. [PubMed]
4. Benninger DH, Georgiadis D, Gandjour J, et al. Accuracy of color duplex ultrasound diagnosis of spontaneous carotid dissection causing ischemia. Stroke. 2006;37:377–81. [PubMed]
5. Dittrich R, Dziewas R, Ritter MA, et al. Negative ultrasound findings with cervical artery dissection. J Neurol. 2006;253(4):424–33. [PubMed]