
{kind=link}
| Author | Affiliation |
|---|---|
| Jason D. Heiner, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, WA |
| Hillary M. Harper, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, WA |
| Todd J. McArthur, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, WA |
An adult male presented to the emergency department complaining of two days of exertional shortness of breath and progressive chest pain. He was afebrile with a blood pressure of 135/88 mmHg, heart rate of 105 beats/minute, respiratory rate of 22 breaths/minute, and a SaO2 of 94% on room air. There was no history of preceding trauma, surgery or known congenital defects. A chest radiograph demonstrated an enlarged cardiac silhouette (Figure 1). Computed tomography revealed the presence of herniated visceral contents within the pericardial sac (Figure 2). Surgery was consulted for operative repair of this intrapericardial diaphragmatic hernia (IPDH), which was causing his presenting symptoms.

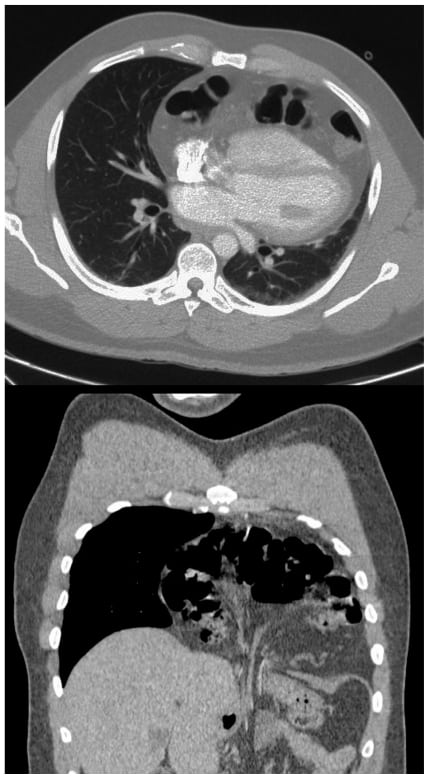
IPDH can occur from a traumatic or congenital diaphragmatic defect of the central tendon. It is a rare complication of diaphragmatic rupture, occurring in less than 1% of cases.1,2 Blunt trauma resulting from automobile collisions has emerged as the most common primary identified cause.3The mechanism in blunt abdominal trauma involves a sudden rise in intra-abdominal pressure, leading to rupture along the right or left side of the diaphragm extending into the pericardium. The organ most frequently involved in traumatic IPDH appears to be the transverse colon, followed by the stomach and the greater omentum.2 Symptoms of IPDH are often nonspecific cardiorespiratory and gastrointestinal complaints. Patients range from being asymptomatic to having potentially fatal cardiac tamponade. The time interval from the presumed origin of the IPDH to the time of diagnosis is quite variable for both traumatic and congenital etiologies.1 Treatment for IPDH is surgical. A thoracic approach is recommended by most authors in cases of delayed IPDH, as this allows for easier removal of pericardial adhesions; whereas, a trans-abdominal approach is preferred for surgical closure in acute presentations to provide good access to the tear in the diaphragm.3
Footnotes
The views expressed herein are solely those of the authors and do not represent the official views of the Department of Defense or Army Medical Department.
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted July 3, 2010; Accepted July 16, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Jason Heiner, MD, Department of Emergency Medicine, Madigan Army Medical Center Tacoma, WA 98431
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Barrett J, Satz W. Traumatic, Pericardio-diaphragmatic rupture: an extremely rare cause of pericarditis. J Emerg Med. 2006;30:141–5. [PubMed]
2. Reina A, Vidaña E, Soriano P, et al. Traumatic intrapericardial diaphragmatic hernia: case report and literature review. Injury. 2001;32:153–6. [PubMed]
3. Sharma OP. Pericardio-diaphragmatic rupture: five new cases and literature review. J Emerg Med.1999;17:963–8. [PubMed]