Author Affiliation Alexander J. Scumpia, DO, MSc Mount Sinai Medical Center, Department of Emergency Medicine, Miami, Florida Daniel A. Aronovich, DO Mount Sinai Medical Center, Department of Emergency Medicine, Miami, Florida Loredana Roman, BS Victor Babes University of Medicine and Pharmacy, Department of Medicine, Timisoara, Romania Vanitha Vasudevan, MD Ryder Trauma Center, Department of Surgery, […]
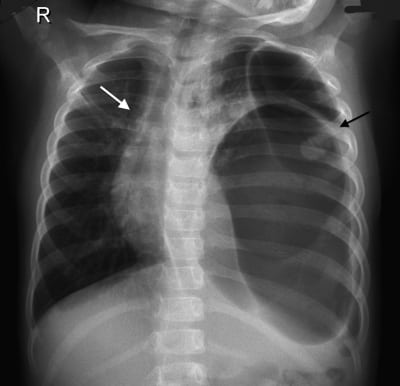
A 4-year-old girl was brought to our hospital by her parents because of abdominal pain. She had suffered minor trauma after rolling from her standard-height bed 2 days prior. Vital signs were appropriate for age. Physical examination was remarkable for decreased breath sounds to the left side of the chest. A chest radiograph (Figure) demonstrated a large gas-filled structure in the left side of the chest with mediastinal shift.
Chilaiditi syndrome, symptomatic interposition of bowel beneath the right hemidiaphragm, is uncommon and usually managed without surgery. Morgagni hernia is an uncommon diaphragmatic hernia that generally requires surgery. In this case a patient with a longstanding diagnosis of bowel interposition (Chilaiditi sign) presented with presumed Chilaiditi syndrome. Abdominal computed tomography was performed and revealed no bowel interposition; instead, a Morgagni hernia was found and surgically repaired. Review of the literature did not reveal similar misdiagnosis or recommendations for advanced imaging in patients with Chilaiditi sign or syndrome to confirm the diagnosis or rule out other potential diagnoses.
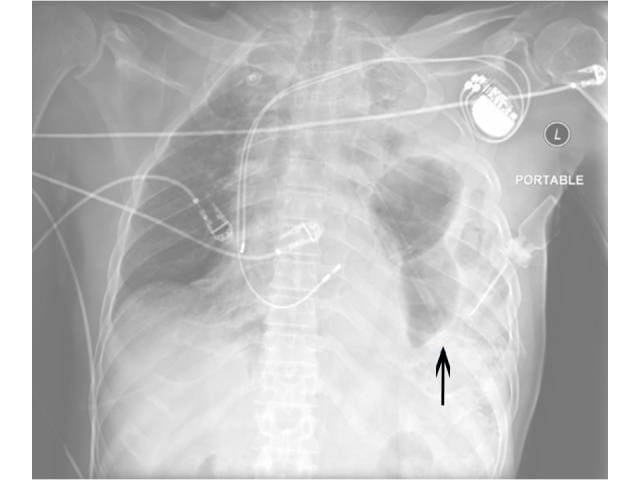
An adult male presented to the emergency department complaining of two days of exertional shortness of breath and progressive chest pain. He was afebrile with a blood pressure of 135/88 mmHg, heart rate of 105 beats/minute, respiratory rate of 22 breaths/minute, and a SaO2 of 94% on room air.
{kind=link}