
{kind=link}
| Author | Affiliation |
|---|---|
| Ross Hooker, MD | Los Angeles County USC Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Ilene Claudius, MD | Los Angeles County USC Medical Center, Department of Emergency Medicine, Los Angeles, California |
| Anh Truong, MD | Los Angeles County USC Medical Center, Department of Emergency Medicine, Los Angeles, California |
ABSTRACT
A 4-year-old girl was brought to our hospital by her parents because of abdominal pain. She had suffered minor trauma after rolling from her standard-height bed 2 days prior. Vital signs were appropriate for age. Physical examination was remarkable for decreased breath sounds to the left side of the chest. A chest radiograph (Figure) demonstrated a large gas-filled structure in the left side of the chest with mediastinal shift.
In the emergency department the patient began exhibiting respiratory distress, and after nasogastric tube insertion, she became bradycardic and hypoxic, and finally lost pulses. The patient underwent intubation and cardiopulmonary resuscitation was initiated. Vigorous suction from the nasogastric tube was initiated, with prompt return of vital signs. The patient recovered well and underwent an operative procedure in which the spleen and part of the stomach and transverse colon were reduced into the abdomen. A 5-cm posterolateral defect in the diaphragm was identified and repaired. The patient left the hospital at neurologic baseline.
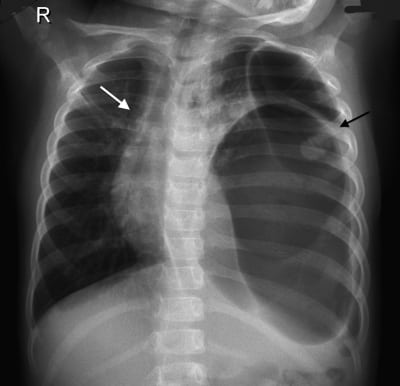
Tension gastrothorax is a rare life-threatening condition occurring when the stomach herniates through a defect in the diaphragm into the chest and becomes distended with air, leading to hemodynamic compromise.1,2 This is seen most commonly in the perinatal period in a patient with a congenital diaphragmatic hernia, or after acute major abdominal trauma or surgery in an otherwise healthy individual, or sometimes years later.2,3 In these settings, diagnosis requires a high level of suspicion, as this will often be mistaken for a tension pneumothorax, a far more common and equally life-threatening condition.1,4 A poorly differentiated diaphragm on chest radiograph, or visualization of a nasogastric tube in the stomach (in the chest), can help differentiate these conditions.2 Tension gastrothorax is treated initially with prompt nasogastric tube placement and vigorous suction of contents and, when stable, intraoperative reduction and repair.1,2
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted April 6, 2011; Accepted April 6, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.4.6763
Address for Correspondence: Ross Hooker, MD
Los Angeles County USC Medical Center, Department of Emergency Medicine, Room 1011, 1200 N State St, Los Angeles, CA 90033
E-mail: rosshooker@hotmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding, sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Slater RG. Tension gastrothorax complicating acute traumatic diaphragmatic rupture. J Emerg Med. 1992;10:25–30. [PubMed]
2. Horst M, Sacher P, Molz G, et al. Tension gastrothorax. J Pediatr Surg. 2005;40:1500–1504.[PubMed]
3. Farhan R, Mallicka MC, Rajeev S, et al. A review on delayed presentation of diaphragmatic rupture.World J Emerg Surg. 2009;4:32. [PMC free article] [PubMed]
4. Nishijima D, Zehbtachi S, Austin RB. Acute posttraumatic tension gastrothorax mimicking acute tension pneumothorax. Am J Emerg Med. 2007;25(734):e5–e6. [PubMed]