
{kind=link}
| Author | Affiliation |
|---|---|
| Jeremy Paulsen, MD | University of Southern California, Los Angeles, CA |
| Nicholas Testa, MD | University of Southern California, Los Angeles, CA |
CASE REPORT
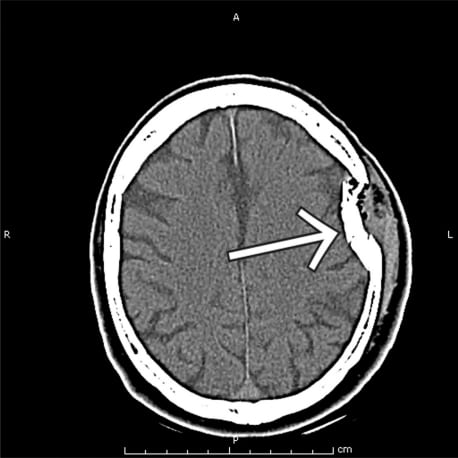
A 59-year-old male presented to the emergency department after having been struck on the head multiple times with a hammer. On presentation, vital signs were all within normal limits and primary exam was only impressive for a large left sided parietal-temporal hematoma. The patient could move all extremities and follow all commands. It was noted, however, that he was not speaking. Initially his aphasia was thought to be volitional, but on further evaluation he appeared frustrated that he was not able to communicate. When provided pen and paper, he was unable to write. A computed tomography of the head was obtained and showed a left-sided depressed skull fracture, as well as underlying subdural bleeding. This patient was urgently taken to the operating room for definitive care. The neurosurgical services followed this patient for two weeks. During that time he was persistently aphasic. He was transferred to a rehabilitation hospital with persistent posttraumatic expressive aphasia.
The importance of this case is to remind the clinician that isolated expressive aphasia can be associated with significant head trauma. A Medline1 search for traumatic aphasia reveals prior case reports of aphasia being the presenting sign of subdural hematomas, but only in the subacute presentation. Other studies have reported the presence of aphasia in major brain trauma to be as high as 19%, although all cases were associated with other significant deficits.2 Most literature focuses instead on the rehabilitation potential in traumatic aphasias, which has been consistently reported to have a much higher success when compared to other causes of aphasia.3,4
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted April 3, 2010; Revision Received July 23, 2010; Accepted September 27, 2010
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Nicholas Testa, MD, 1200 North State St, Room 1011, Los Angeles, California 90033
Email: testa@usc.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Dell SO, Batson R, Kasdon DL, et al. Aphasia in subdural hematoma. Arch Neurol. 1983 Mar;40(3:):177–9. [PubMed]
2. Safaz I, Alaca R, Yasar E, et al. Medical complications, physical function and communication skills in patients with traumatic brain injury: a single centre 5-year experience. Brain Inj. 2008 Sep;22(10:):733–9. [PubMed]
3. Dayer A, Roulet E, Maeder P, et al. Post-traumatic mutism in children: clinical characteristics, pattern of recovery and clinicopathological correlations. Eur J Paediatr Neurol. 1998;2(3):109–16.[PubMed]
4. Groher M. Language and memory disorders following closed head trauma. J Speech Hear Res.1977 Jun;20(2:):212–23. [PubMed]