
{kind=link}
| Author | Affiliation |
|---|---|
| Thomas W. Quimby, MD | Maine Medical Center, Department of Emergency Medicine, Portland, ME |
| Ariel A. Clark, MD | Maine Medical Center, Department of Emergency Medicine, Portland, ME |
| Megan L. Fix, MD | Maine Medical Center, Department of Emergency Medicine, Portland, ME |
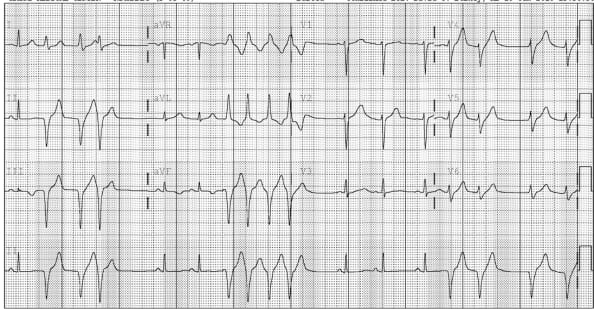
A healthy 26 year-old G3P2 12 weeks pregnant with twins presented to the emergency department after the abrupt onset of palpitations, dizziness, shortness of breath and chest pain. An initial electrocardiogram demonstrated frequent preventricular contractions, which progressed to runs of sustained ventricular tachycardia (VT) [Figure 1]. Further workup, including blood work, a computed tomography of the chest and an echocardiogram, was negative for electrolyte imbalance, pulmonary embolism and structural heart disease. The arrhythmia was eventually terminated with verapamil, and she was discharged symptom free five days later on oral metoprolol.
Of patients presenting with monomorphic VT, 90% of cases are secondary to structural heart disease, including ischemic heart disease, congenital heart disease, valvular dysfunction and myocardial dysfunction.1,2 The remaining 10% are referred to as “idiopathic” VT, as they represent VT in the absence of identifiable structural disease.1,2 Seventy-five to 90% of idiopathic VT originates in the right ventricle, while the remaining cases represent an ectopic focus within the left ventricle, especially the left posterior fascicle.1 This rare arrhythmia of the left ventricle was first described as a unique electrophysiologic entity in 1981 by Belhassen et al. Commonly referred to as fascicular or intrafascicular tachycardia, verapamil sensitive VT or Belhassen VT, it is characterized by a right bundle branch block pattern and left axis deviation.3 Patients are typically young and healthy with their first episode often occurring in adolescence.2 Attacks may be precipitated by exercise, excitement, and infection.2 Patients usually present with palpations, dizziness, fatigue, and shortness of breath but are typically hemodynamically stable.1,2 The prognosis is excellent and the incidence of syncope and sudden death is rare.1,2 Intravenous verapamil has proven efficacious for terminating VT in symptomatic patients.3 Patients with recurrent refractory episodes of VT may be referred for radiofrequency ablation.1,2
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Submission history: Submitted April 11, 2010; Accepted April 19, 2010.
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Megan L. Fix, MD, Maine Medical Center, Department of Emergency Medicine, 47 Bramhall Street, Portland, ME 04102
Email: meganfix@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Chiu C, Sequeira IB. “Diagnosis and Treatment of Idiopathic Ventricular Tachycardia.” AANC Clinical Issues. 2004;15(3):449–61.
2. Topilski I, Glick A, Belhassen B. “Idiopathic Left Ventricular Tachycardia with a Right Bundle Branch Block Morphology and a Left Axis Deviation (“Belhassen type”): Results of Radiofrequency Ablation in 18 Patients” Isr Med Assoc J. 2004;6:195–200. [PubMed]
3. Belhassen B, Rotmensch HH, Laniado S. “Response of Sustained Recurrent Ventricular Tachycardia to Verapamil” Br Hear J. 1981;46:679–82.