
{kind=link}
| Author | Affiliation |
|---|---|
| Browning S. Wayman, MD, DTM&H | University of Texas Health Science Center at San Antonio, Department of Emergency Medicine, San Antonio, Texas |
| Ryan Joseph, DO, DTM&H | University of Texas Health Science Center at San Antonio, Department of Emergency Medicine, San Antonio, Texas |
ABSTRACT
Case Presentation
We present a case of a 59-year-old male who presented to the emergency department with left upper arm pain that started suddenly after lifting some plywood a few days prior. Point-of-care ultrasound (POCUS) was performed, which revealed a rupture of the long head of the biceps tendon.
Discussion
Biceps tendon rupture is a relatively rare occurrence; however, rupture of the long head is more common than the short head. Being competent in bedside musculoskeletal POCUS is important for the emergency physician and can help expedite care in cases such as the one presented here.
CASE PRESENTATION
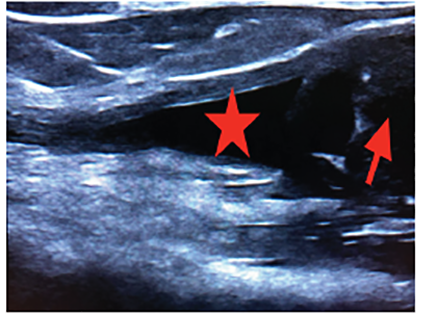
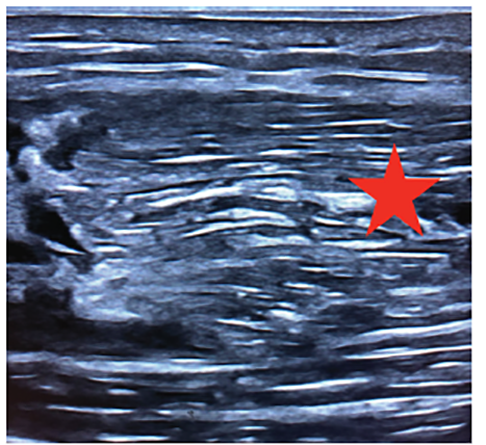
A 59-year-old male presented to the emergency department with left upper arm pain, which began abruptly while lifting some plywood about six days prior. On examination, he had significant tenderness at the proximal biceps and significant pain with passive range of motion as well as three out of five strength. There was also a large, soft tissue defect at his proximal bicep with ecchymosis. Point-of-care ultrasound (POCUS) revealed a proximal rupture of the long head of the biceps tendon (LHBT) (Images 1–3).

DISCUSSION
Biceps tendon rupture is a relatively rare occurrence with a reported incidence rate of 0.53/100,000 over a period of five years, with a male to female ratio of 3:1.1 These injuries are more likely to occur in middle age, and associated risk factors include smoking, corticosteroids, overuse, and diabetes. Proximal biceps tendon rupture is more common than distal and usually occurs at the tendon labral junction or the bony attachment.2 Also, rupture of the LHBT is far more common than rupture of the short head.3
Musculoskeletal ultrasound enables the clinician to perform a dynamic exam at bedside and has a sensitivity and specificity of 88% and 98%, respectively.4 In this case, the emergency physician was able to diagnose a complete proximal LHBT rupture via clinical exam and confirmation with POCUS.
CPC-EM Capsule
What do we already know about this clinical entity?
Biceps tendon rupture is an uncommon injury that usually occurs when the long head biceps tendon is torn. It has traditionally been a clinical diagnosis.
What is the major impact of the image(s)?
These ultrasound images will aid in identifying the anatomy of a ruptured long head of the biceps tendon.
How might this improve emergency medicine?
Familiarity with musculoskeletal ultrasound can hasten diagnosis in the emergency department and appropriate follow-up.
Footnotes
Section Editor: Shaddi Lahham, MD, MS
Full text available through open access at http://escholarship.org/uc/uciem_cpcem
The authors attest that their institution requires neither Institutional Review Board approval, nor patient consent for publication of this image in emergency medicine. Documentation on file.
Address for Correspondence: Ryan Joseph, DO, DTM&H, University of Texas Health Science Center at San Antonio, Department of Emergency Medicine, 7703 Floyd Curl Dr. MC 7736, San Antonio, TX 78229. Email: josephr1@uthscsa.edu. 4:493 – 494
Submission history: Revision received April 18, 2020; Submitted June 25, 2020; Accepted July 3, 2020
Conflicts of Interest: By the CPC-EM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 2008;39(12):1338.
2. Hsu D, Anand P, Chang KV. Biceps tendon rupture. 2020.
3. Shah AK, Pruzansky ME. Ruptured biceps brachii short head muscle belly: a case report. J Shoulder Elbow Surg. 2004;13(5):562-5.
4. Skendzel JG, Jacobson JA, Carpenter JE, et al. Long head of biceps brachii tendon evaluation: accuracy of preoperative ultrasound. AJR Am J Roentgenol. 2011;197(4):942-8.