
{kind=link}
| Author | Affiliation |
|---|---|
| Giora Weiser, MD | Rambam Health Care Campus, Meyer Children’s Hospital, Rambam Health Care Campus, Haifa, Israel |
| Nira Beck-Razi, MD | Rambam Health Care Campus, Department of Medical Imaging, Haifa, Israel |
| Itai Shavit, MD | Rambam Health Care Campus, Meyer Children’s Hospital, Rambam Health Care Campus, Haifa, Israel |
ABSTRACT
We report on a 3-month-old infant, who arrived in the pediatric emergency department (ED) with a cervical cystic hygroma causing an impending compromise of the airway. We recognize that such a lesion can rapidly progress, and the judicious use of imaging in the ED may help to avoid airway compromise and possibly fatal complications.
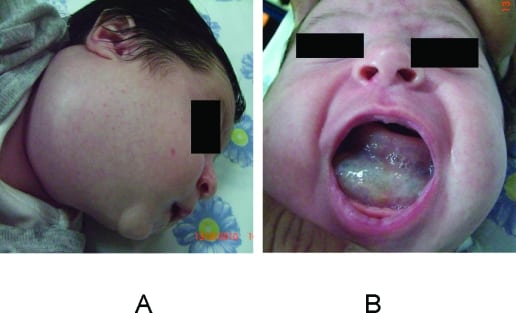
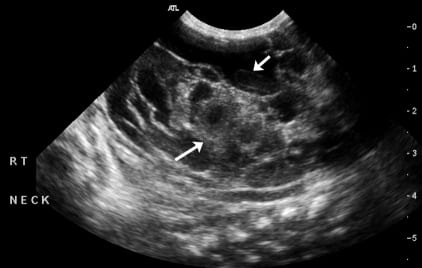
A 3-month-old boy, who was diagnosed after birth as having a cystic hygroma, was referred to the emergency department (ED) for further evaluation. The baby had no signs of respiratory distress, but a large lesion was noticed on the right neck, emerging from the base of the tongue and threatening the airway patency (Figure 1). Ultrasound examination revealed a large cystic lesion insinuating around the normal structures of the neck on both sides without compressing the airway (Figure 2). The patient was admitted for further evaluation, and a prophylactic tracheotomy was performed. Unfortunately, the baby died at home 2 months later because of tracheotomy tube–related complications.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted January 1, 2011; Revision received January 14, 2011; Accepted February 7, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.2.2170
Address for Correspondence: Itai Shavit, MD
Rambam Health Care Campus, Meyer Children’s Hospital, Department of Emergency Medicine, 6 Ha’Aliya St, PO Box 9602, Haifa 31096, Israel
E-mail: itai@pem-database.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Fordham LA, Chung CJ, Donnely LF. Imaging of congenital vascular and lymphatic anomalies of the head and neck. Neuroimaging Clin North Am. 2000;;10:117–136.
2. Sannoh S, Quezada E, Merer DM, et al. Cystic hygroma and potential airway obstruction in a newborn: a case report and review of the literature. Cases J. 2009;;2:48. [PMC free article] [PubMed]
3. Thompson DM, Kasperbauer JL. Congenital cystic hygroma involving the larynx presenting as an airway emergency. J Natl Med Assoc. 1994;;86:629–632. [PMC free article] [PubMed]
4. Perkins JA, Manning SC, Tempero RM, et al. Lymphatic malformations: review of current treatment. Otolaryngol Head Neck Surg. 2010;;142:795–803. [PubMed]
5. Luzzatto C, Midrio P, Tchaprassian Z, et al. Sclerosing treatment of lymphangiomas with OK-432.Arch Dis Child. 2000;;82:316–318. [PMC free article] [PubMed]
6. Ishaq M, Minhas MR, Hamid M, et al. Management of compromised airway due to unusual presentation of cystic hygroma. J Pak Med Assoc. 2006;;56:135–137. [PubMed]
7. Barrand KG, Freeman NV. Massive infiltrating cystic hygroma of the neck in infancy. Arch Dis Child. 1973;;48:523–531. [PMC free article] [PubMed]
8. Sheth S, Nussbaum AR, Hutchins GM, et al. Cystic hygromas in children: sonographic-pathologic correlation. Radiology. 1987;;162:821–824. [PubMed]