
{kind=link}
| Author | Affiliation |
|---|---|
| Lee W. Shockley, MD, MBA | Denver Health Medical Center, The University of Colorado School of Medicine |
| John L. Kendall, MD | Denver Health Medical Center, The University of Colorado School of Medicine |
ABSTRACT
We present the case of a 31-year-old trauma patient with computed tomography concerning significant C3–C4 subluxation. The abnormality is due to an artifact with which emergency physicians should be aware.
A 31-year-old woman fell from a van traveling between 20–40 miles per hour. She briefly lost consciousness. She was immobilized on a backboard with towel rolls and tape because a standard extrication collar would not fit. The patient was confused and agitated with a Glasgow Coma Scale of 12. She moved all four extremities and had a large posterior scalp laceration. Computed tomography (CT) of her head was normal except for the laceration. The sagittal reconstruction of her cervical spine CT is shown (Figure 1).

The image was initially interpreted as a 4 mm of subluxation of C3 on C4. This was consistent with the presumed hyperflexion mechanism of injury. Physiologic subluxation of C2 on C3 is a normal finding in up to 9% of children under age seven years.1, 2 This is probably due to immature muscular development and hypermobile spines. There is at least one published report of an adult with C2 on C3 pseudosubluxation.3 However, C3 on C4 subluxation is always considered abnormal (Figure 2).
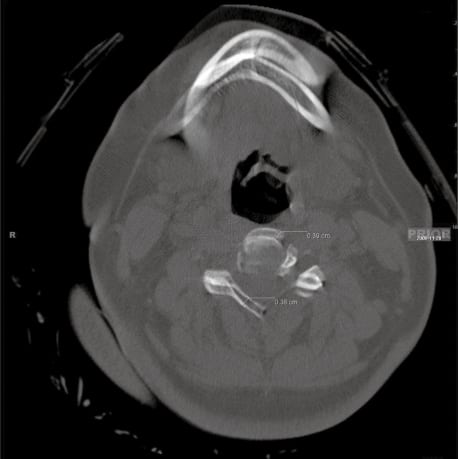
There are clues of a movement artifact on this image, such as the lack of soft tissue swelling, a sharply irregular line of the posterior pharynx, and an oddly shaped mandible. Examination of the axial image at the C3–C4 area revealed that the patient moved 4mm and assumed a new position for the remainder of the study. Recognition of this movement artifact is important in the accurate evaluation of spine CT scans.
CONCLUSION
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted: August 18, 2010; Accepted August 23, 2010.
Reprints available through open access at http://escholarship.org/uc/uciem_westjem.
Address for Correspondence: Lee W. Shockley, MD, MBA, Denver Health Medical Center, The University of Colorado School of Medicine
Email: Lee.Shockley@dhha.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Betz RR, Mulcahey MJ, D’Andrea LP, et al. Acute evaluation and management of pediatric spinal cord injury. J Spinal Cord Med. 2004;27(Suppl 1):S11–5. [PubMed]
2. Shaw M, Burnett H, Wilson A, et al. Pseudosubluxation of C2 on C3 in polytraumatized children–prevalence and significance. Clin Radiol. 1999 Jun;54(6):377–80. [PubMed]
3. Curtin P, McElwain J. Assessment of the “nearly normal” cervical spine radiograph: C2–C3 pseudosubluxation in an adult with whiplash injury. Emerg Med J. 2005 Dec;22(12):907–8.[PMC free article] [PubMed]