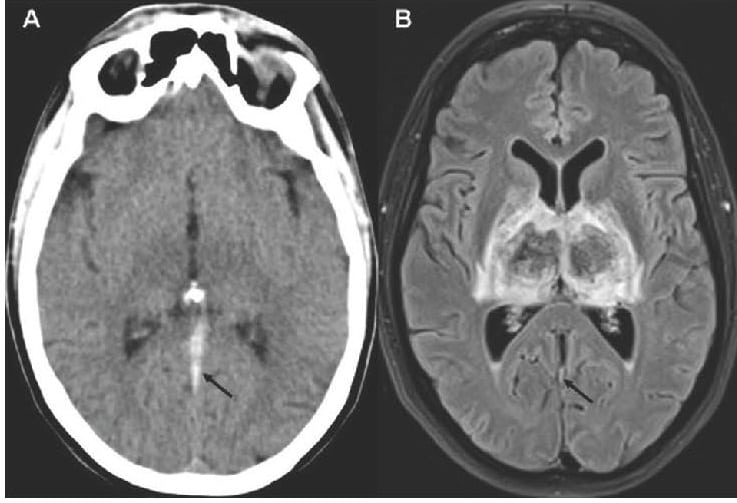
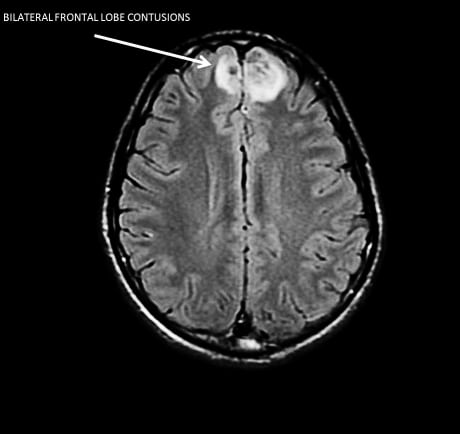
A 35-year-old woman, without previous medical history except oral contraception, presented with sudden onset of stupor and clonic perseveration in the upper limbs. She was aphasic, but communicated by vertical movements of the head. Unenhanced brain computed tomography (CT) demonstrated…
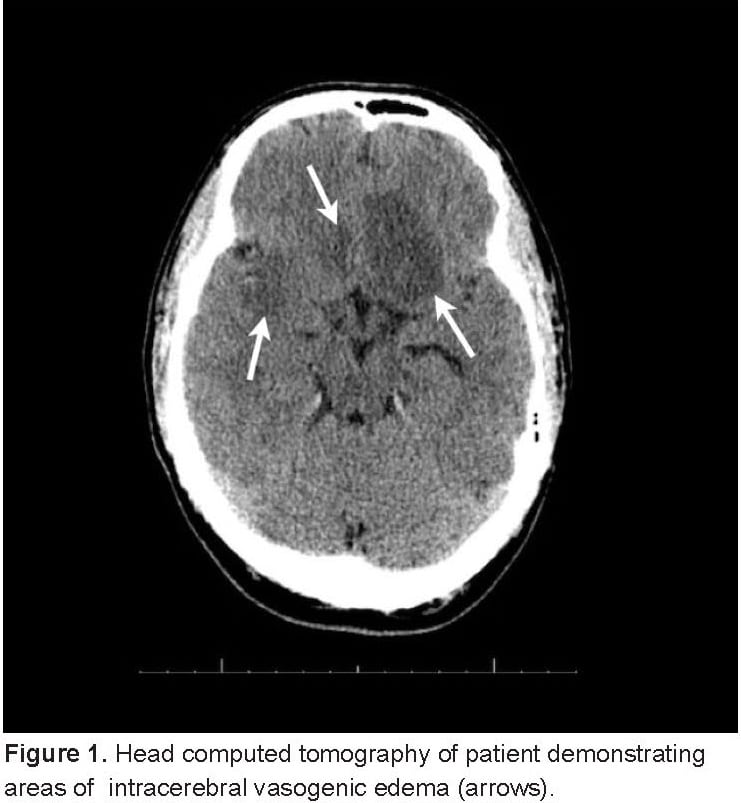
We report a case of altered mental status secondary to acute Toxoplasma Gondii encephalitis. The patient had no medical or surgical history and presented with acute onset of lethargy with no clear precipitant. A physical exam revealed no focal neurological deficits and a subsequent medical workup revealed multiple intracranial lesions with a biopsy confirming the diagnosis of Toxoplasma Gondii encephalitis in the setting of newly diagnosed human immunodeficiency virus (HIV). A literature review revealed that this is a unique case of toxoplasmic encephalopathy in the United States in a previously undiagnosed HIV positive patient presenting to an emergency department.
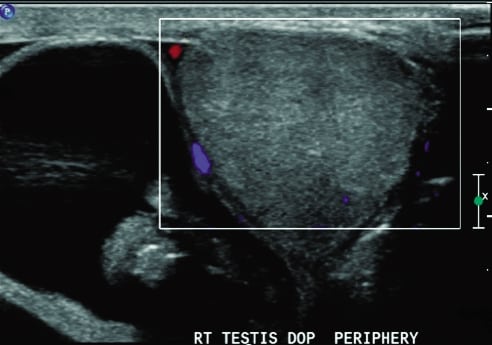
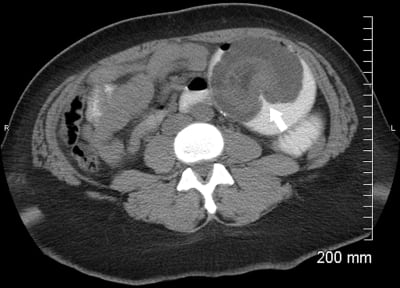
A 34-year-old male presented to the emergency department with a 3-hour complaint of pain in the right lower quadrant and right testicle. He stated that his pain began suddenly while standing at work. On physical examination, he had a small, firm, unreducible bulge in his right inguinal canal and an enlarged right scrotum. The patient was placed in trendelenburg position; intravenous fentanyl, valium, and dilaudid were administered; and surgery consult was obtained. A testicular ultrasonogram (Figure) was obtained owing to continued pain in the right scrotum and inability to evaluate the testicle. After viewing the ultrasound pattern, the patient was promptly taken to the operating room 6 hours after onset of symptoms.
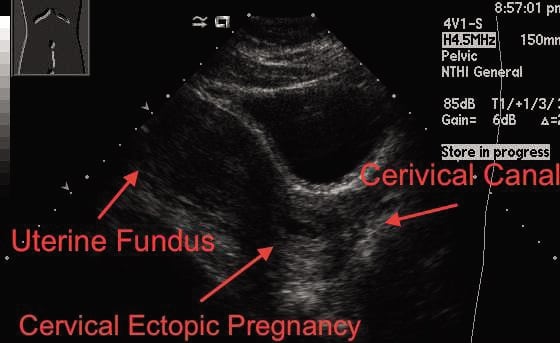
A 31-year-old, who is gravida 2 para 1 at 6 weeks by last menstrual period, presents for vaginal bleeding starting approximately 5 days earlier. The bleeding was initially light, and there was no associated abdominal pain. The bleeding seemed to stop when she laid down and increased upon standing.
Internuclear ophthalmoplegia is a rare condition caused by injury to the medial longitudinal fasciculus in the brainstem. It usually occurs in conditions such as stroke or multiple sclerosis and is extremely rare after head injury. We report a case of unilateral internuclear ophthalmoplegia, which occurred after a minor head injury in a young male. His only symptoms were headache and diplopia. He was treated conservatively, and his symptoms settled after 3 months.
A 58-year-old female presented to the emergency department (ED) with pain and swelling to the right arm after receiving propofol during an outpatient procedure for nasal polyps.
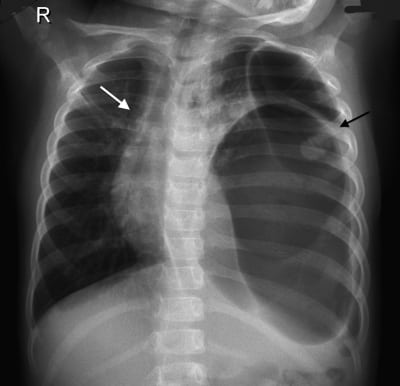
A 4-year-old girl was brought to our hospital by her parents because of abdominal pain. She had suffered minor trauma after rolling from her standard-height bed 2 days prior. Vital signs were appropriate for age. Physical examination was remarkable for decreased breath sounds to the left side of the chest. A chest radiograph (Figure) demonstrated a large gas-filled structure in the left side of the chest with mediastinal shift.
A 68-year-old male with moderate mental retardation presented to the emergency department with anorexia, constipation, and abdominal distension for 4 days. Medical history was significant for partial colon resection for presumed bowel obstruction 3 years previously (no true anatomic cause for obstruction was identified at surgery).
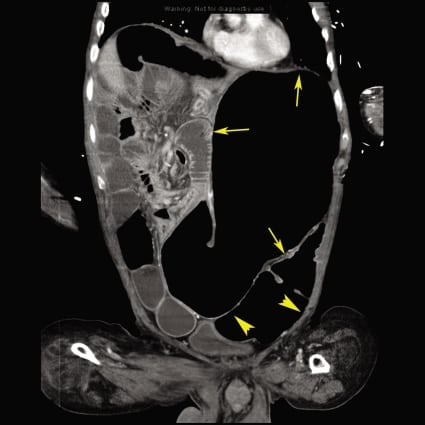
A 38-year-old female presented with acute onset epigastric abdominal pain and vomiting. Surgical history included gastric bypass surgery 8 years prior and cesarean delivery. The patient was in severe distress, afebrile, had significant epigastric tenderness with guarding, normal bowel sounds, and no distention or masses.
A 52-year-old Caucasian male presented to the emergency department complaining of nontraumatic painful swelling and redness of the distal left fourth finger for 2 days, associated with malaise and subjective fever. The patient denied medical history, drugs, tobacco, or alcohol use.
A 43-year-old man presented to the emergency department after he was swimming in the ocean and felt a sudden sting followed by a burning pain and muscle spasms in his right hand.
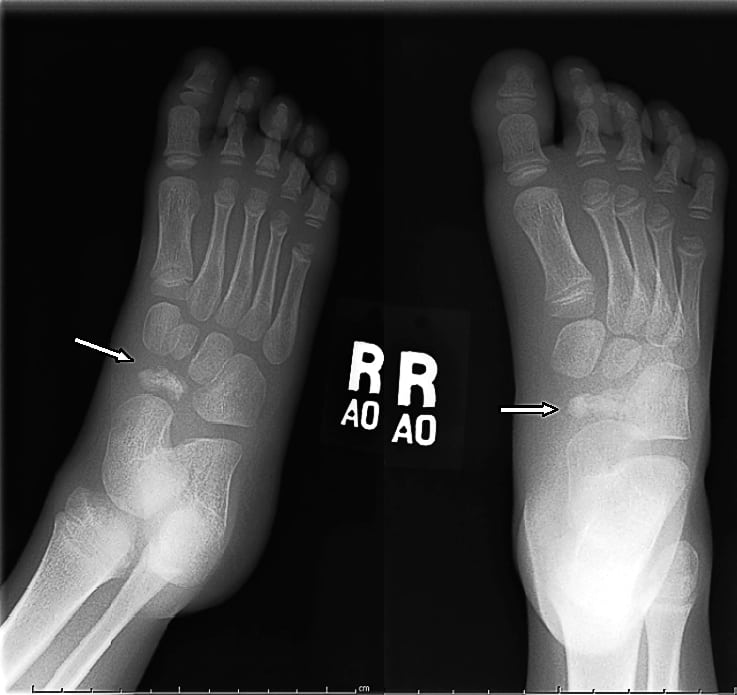
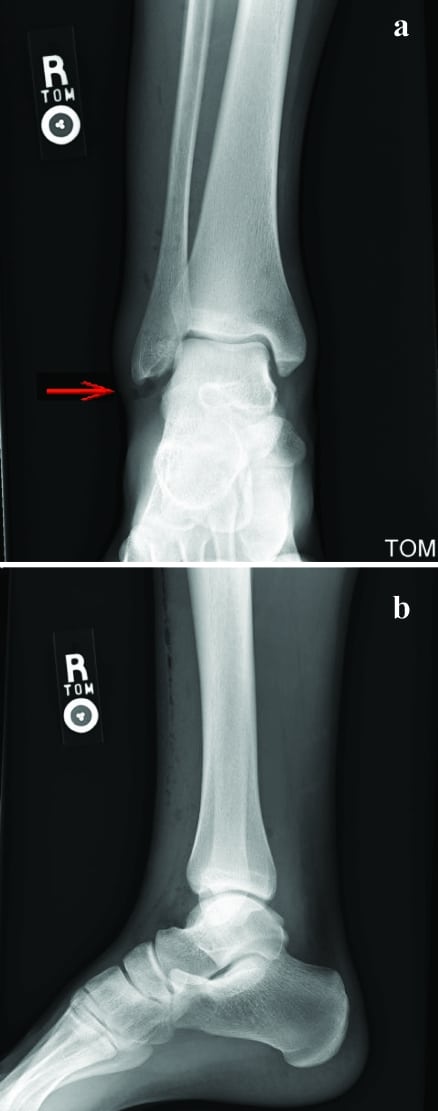
A healthy 19-year-old male presented with complaints of right ankle pain. Twelve hours before, he had jumped off a skateboard, inverting and abrading his right ankle.
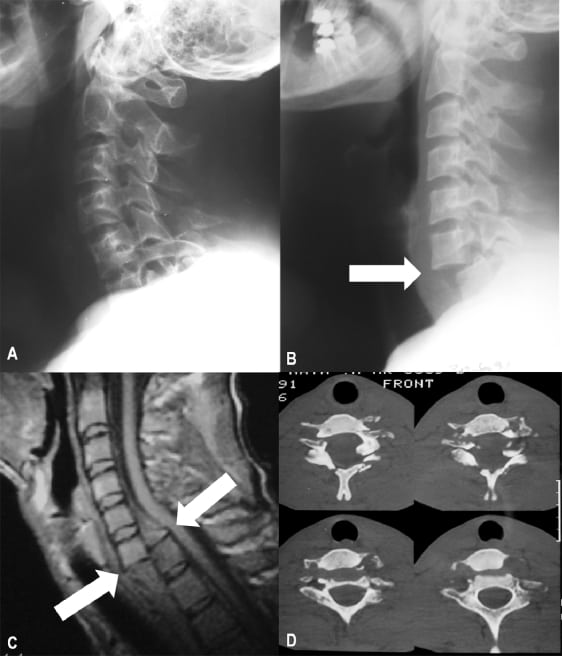
A 30-year-old man presented to the emergency department after a motorcycle accident at high speed. He reported neck pain and referred paresthesia along the fourth and fifth fingers of both the left and the right hand. The patient arrived at hospital hemodynamically stable.
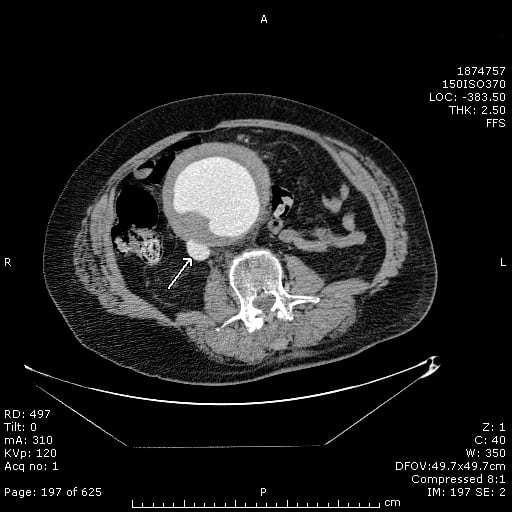
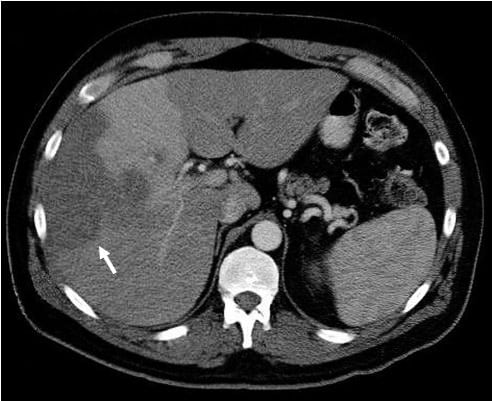
We present a case of pylephlebitis, which is an infective suppurative thrombosis of the portal vein. Pylephlebitis is an uncommon complication of intra-abdominal infections and carries with it significant morbidity and mortality.
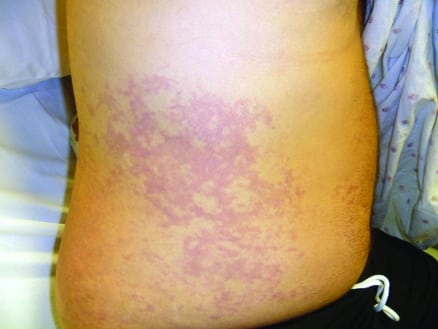
A 29-year-old man presented to the emergency department (ED) with a rash across his chest and abdomen. The rash began 2 hours before his arrival and was initially pruritic, but subsequently became painful. The patient also complained of acute onset of aching pain in both hips and his left arm. He denied associated chest pain or dyspnea, and had no paresthesias or disequilibrium. Routine laboratory studies and chest radiograph were normal. Earlier in the day, the patient had completed a dive to 235 feet in depth in Lake Mead, Nevada, but reported a very controlled ascent with appropriate decompression stops. Two days earlier, he had completed a dive to 315 feet in Lake Mead without any problems.
An 11-year-old female presented to the emergency department with fever of 1 day’s duration and sore throat. Her family described a 3-week history of cough with fever, trouble breathing, and wheezing.
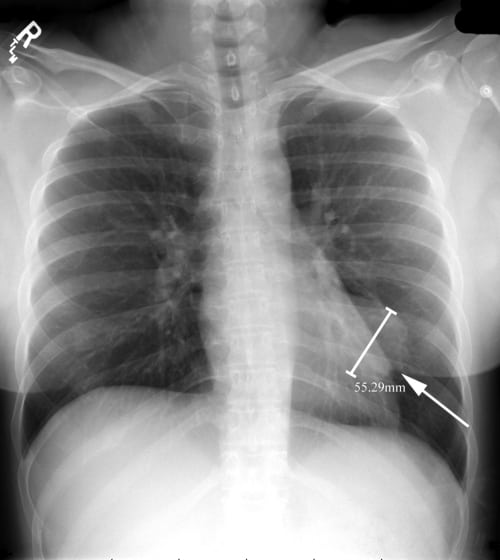
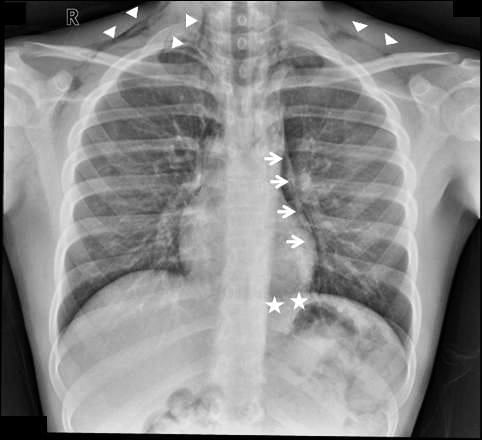
Although pneumomediastinum (PM) is a cause of chest pain, which can be diagnosed on a plain chest radiograph, emergency physicians frequently miss the diagnosis. As follows a description of findings of PM on a chest radiograph.
A 40-year-old male with human immunodeficiency virus (currently, CD4 171) presented to our emergency department (ED) with pain and swelling in the left third digit of 3 to 4 weeks’ duration. He noticed the swelling after a fist fight that resulted in compression of his ring on the finger.
A 35-year-old man presented to the emergency department complaining of right hip pain after being struck by a car while crossing the road. His vital signs were stable, and he complained of right hip pain. He had no other comorbidity. On examination, tenderness and reduced abduction were noted in his right hip, but the gait was normal.
{kind=link}