
{kind=link}
| Author | Affiliation |
|---|---|
| Negean Afifi, DO | Cook County Hospital (Stroger), Department of Emergency Medicine, Chicago, Illinois |
| Jenny J Lu, MD, MS | Cook County Hospital (Stroger), Department of Emergency Medicine, Chicago, Illinois |
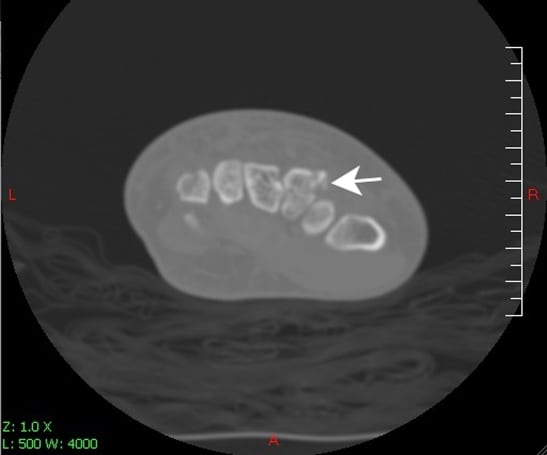
A 45-year-old woman presented to the emergency department with left wrist pain following a fall. Physical exam was remarkable for soft tissue swelling of the palmar and dorsal hand, point tenderness at the base of the second metacarpal, and limited active range of motion. Three-view wrist radiographs showed significant soft tissue swelling without evidence of fracture or dislocation. Computed tomography obtained due to concern for an occult fracture revealed a comminuted fracture of the trapezoid bone involving the articular surface with an anteriorly displaced bone fragment (Figures 1 and 2). The patient was placed in a sugar-tong splint and given orthopedic follow up.

Fractures of the trapezoid bone are rare, accounting for 0.4% of carpal fractures.1 This is primarily due to its protected position in the wrist, nestled within strong intercarpal ligaments between the surrounding carpal bones and the base of the second metacarpal. Its position and integrity contribute vitally to the carpal arch, but make detection of injury elusive.1,2 Fractures are rarely isolated, often involving fractures of the second metacarpal base.2 Patients may have second metacarpal base tenderness, “snuffbox” tenderness,3 or pain with axial loading of the second digit4after trauma involving an axial or bending force along the second metacarpal. The overlapping bones and intimate articulations of the wrist make plain radiographs difficult to interpret.1,5 In 2 separate reports reviewing 17 trapezoid fractures, only 1 fracture was diagnosed by plain radiographs; all others required advanced imaging.6,7 In 1 study, 30% of wrist fractures missed by plain radiograph were diagnosed by computed tomography.5 Treatment approaches have varied from cast immobilization to open reduction and internal fixation, depending on degree of displacement and integrity of the carpal arch.1,6 Unrecognized trapezoid fractures may lead to functional compromise. Delayed union and nonunion resulting in diminished grasp power2 and pain are reported.2,4,8 In a patient with the appropriate mechanism, persistent pain, or second metacarpal base injuries, it falls on the emergency physician to suspect and diagnose this fracture.2,8
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted January 18, 2011; Revision received March 3, 2011; Accepted March 21, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.3.2202
Address for Correspondence: Jenny J. Lu, MD, MS
Cook County Hospital (Stroger), Department of Emergency Medicine, 1900 W Polk St, 10th Floor, Chicago, IL 60612
E-mail: jlu@cookcountyhhs.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Papp S. Carpal bone fractures. Orthop Clin N Am. 2007;;38:251–260.
2. Watanabe H, Hamada Y, Yamamoto Y. A case of old trapezoid fracture. Arch Orthop Trauma Surg.1999;;119:356–357. [PubMed]
3. Jeong GK, Lester B. Isolated fracture of the trapezoid. Am J Orthop. 2001;;30:228–230. [PubMed]
4. Nagumo A, Toh S, Tsubo K, et al. An occult fracture of the trapezoid bone: a case report. J Bone Joint Surg Am. 2002;;84:1025–1027. [PubMed]
5. Welling R, Jacobson J, Jamadar D, et al. MDCT and radiography of wrist fracture: radiographic sensitivity and fracture patterns. Am J Rad. 2008;;190:10–16.
6. Gruson K, Kaplan K, Paksima N. Isolated trapezoid fractures: a case report with compilation of the literature. Bull NYU Hosp Jt Dis. 2008;;66:57–60. [PubMed]
7. Brismar J. Skeletal scintigraphy of the wrist in suggested scaphoid fracture. Acta Radiol.1988;;29:101–107. [PubMed]
8. Sadowski R, Montilla R. Rare isolated trapezoid fracture: a case report. Hand. 2008;;3:372–374.[PMC free article] [PubMed]