
{kind=link}
| Author | Affiliation |
|---|---|
| Eric R Schmitt, MD, MPH | Harbor–UCLA Medical Center, Department of Emergency Medicine, Torrance, California |
| Michael D Burg, MD | Kaweah Delta Medical Center, Department of Emergency Medicine, Visalia, California |
An 11-year-old female presented to the emergency department with fever of 1 day’s duration and sore throat. Her family described a 3-week history of cough with fever, trouble breathing, and wheezing. Her medical history included panhypopituitarism and asthma, and she was receiving steroid replacement therapy. She had recently undergone a dental extraction. Examination showed a temperature of 39.5°C, a 3/6 systolic murmur, bibasilar rales, and palpable cervical subcutaneous emphysema. On chest radiograph, the diaphragm appeared continuous and was not obscured by the inferior heart border (Figure 1). A computed tomography scan demonstrated the same finding (Figure 2).
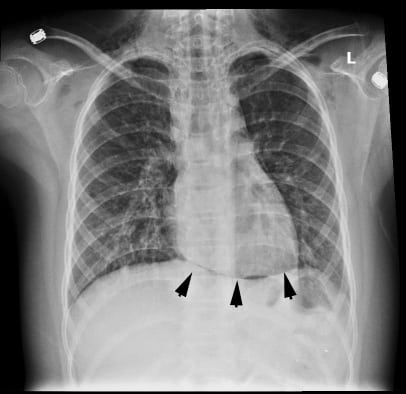

The images depict a “continuous diaphragm sign,” an infrequent indicator of pneumomediastinum.1It is seen on a frontal radiograph when gas in the mediastinum separates the heart and the superior surface of the diaphragm, and it can be seen on either upright or supine views.1,2 A continuous diaphragm may also be seen with pneumopericardium, although it is much less common.3,4Distinguishing the 2 conditions radiographically can be challenging, but pneumopericardium typically appears as an isolated broad band around the heart rather than the multiple thin lucent streaks extending into neck seen with pneumomediastinum.3
Pneumomediastinum occurs after alveolar rupture as gas travels along the bronchovascular interstitial sheaths into the mediastinum.3,5 Nontraumatic causes include invasive procedures and mechanical ventilation, airway obstruction, barotrauma, and pulmonary or pericardial infections, and it has also been described after dental extractions.3–6 Spontaneous pneumomediastinum is rare and usually benign, and tends to occur in males and younger patients.7,8 Common symptoms of pneumomediastinum are chest pain and dyspnea, and signs are subcutaneous emphysema, wheezing, and Hammon sign.3,7,8 Differential diagnoses include pneumothorax and esophageal rupture, and complications include hypotension from impaired venous return, tension pneumothorax, and cardiac tamponade.3,4,7
Most cases follow a benign course and require no therapy, although in 1 series prophylactic antibiotics were given and all cases resolved without complication.8
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted April 12, 2011; Revision received April 20, 2011; Accepted April 25, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.4.2283
Address for Correspondence: Eric R. Schmitt, MD, MPH
Harbor–UCLA Medical Center, Department of Emergency Medicine, 1000 W Carson St, Box 21, Torrance, CA 90509
E-mail: ericrschmitt@yahoo.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Levin B. The continuous diaphragm sign: a newly-recognized sign of pneumomediastinum. Clin Radiol. 1973;;24:337–338. [PubMed]
2. MacPherson P, Davidson JS. Letter: continuous diaphragm sign of pneumomediastinum. Br Med J.1974;;2:119–120. [PMC free article] [PubMed]
3. Bejvan SM, Godwin JD. Pneumomediastinum: old signs and new signs. Am J Roentgenol.1996;;166:1041–1048. [PubMed]
4. Brander L, Ramsay D, Dreier D, et al. Continuous left hemidiaphragm sign revisited: a case of spontaneous pneumopericardium and literature review. Heart. 2002;;88:e5. [PMC free article][PubMed]
5. Zylak CM, Standen JR, Barnes GR, et al. Pneumomediastinum revisited. Radiographics.2000;;20:1043–1057. [PubMed]
6. Gurjar M, Chaudhary A, Poddar B, et al. “Continuous diaphragm sign” after endotracheal intubation. Pediatr Emerg Care. 2010;;26:68–69. [PubMed]
7. Bullaro FM, Bartoletti SC. Spontaneous pneumomediastinum in children: a literature review.Pediatr Emerg Care. 2007;;23:28–30. [PubMed]
8. Miura H, Taira O, Hiraguri S, et al. Clinical features of medical pneumomediastinum. Ann Thorac Cardiovasc Surg. 2003;;9:188–191. [PubMed]