
{kind=link}
| Author | Affiliation |
|---|---|
| Radhika Sundararajan, MD, PhD | Brigham and Women’s Hospital, Department of Emergency Medicine, Boston, Massachusetts |
| Adam B Landman, MD | Brigham and Women’s Hospital, Department of Emergency Medicine, Boston, Massachusetts |
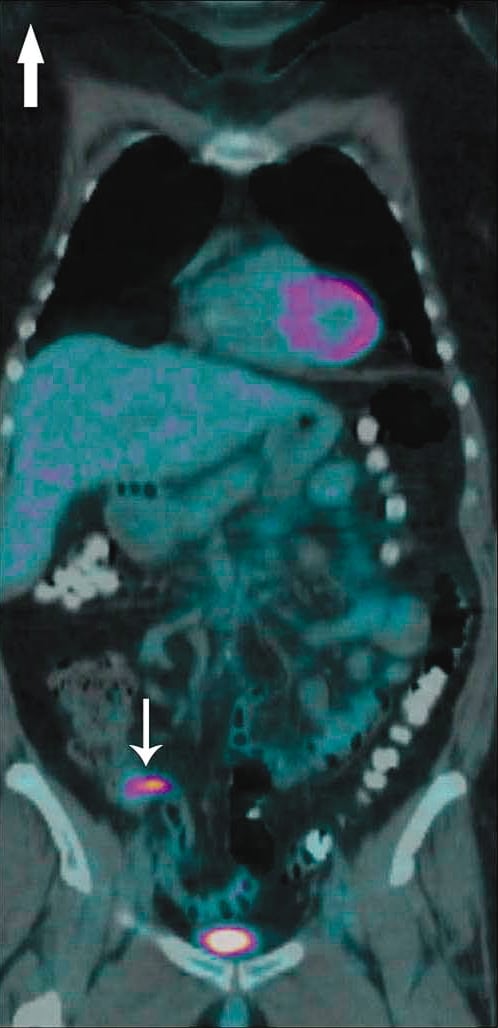
A 62-year-old female presented to the emergency department (ED) with right lower quadrant pain for 3 days. Past medical history was notable for small cell lung cancer (SCLC) with brain metastases. A staging positron emission tomography (PET) performed 10 days prior to presentation showed fludeoxyglucose uptake in the proximal appendix without surrounding inflammation (Figure 1).
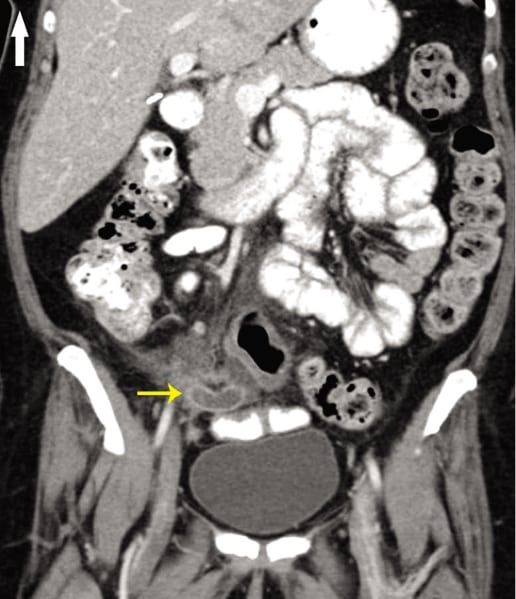
In the ED, her physical exam was notable only for right lower quadrant tenderness to palpation, without rebound or guarding. Vital signs were within normal limits. Laboratory results were notable for a white blood count of 22 K/uL with 94% neutrophils (<5% bands). Contrast-enhanced abdominal computed tomography (CT) was performed in the ED showing a dilated appendix with enhancing wall and surrounding fat stranding suggestive of acute appendicitis (Figure 2). She was taken to the operating room emergently for a laproscopic appendectomy, which revealed a perforated appendix. The patient did well and 1 week postoperatively resumed treatment for her SCLC.
Pathology of the appendiceal specimen demonstrated oval cells and nuclear molding consistent with small cell carcinoma involving the musclaris propria.
Malignancies are a rare but known cause of appendiceal obstruction and inflammation, most commonly primary tumors, such as carcinoid or adenocarcinoma. This case of appendicitis from metastatic SCLC is exceedingly more rare, with only 7 prior case reports documented.1,2Interestingly, this patient also had a staging PET CT that detected the metastasis prior to appendiceal obstruction and symptom onset. Other case reports have described screening PET CT incidentally diagnosing acute appendicitis.3,4
While metastases are an uncommon cause of appendiceal obstruction and inflammation, they should be considered as part of the differential diagnosis when a patient with known malignancy presents with symptoms consistent with appendicitis.
ACKNOWLEDGMENTS
The authors would like to thank Gamaliel Rodriguez-Hernandez, MD, and Pamela Deavers, MD, from the Brigham and Women’s Hospital Department of Radiology and Brooke Lane, MD, from the Brigham and Women’s Hospital Department of Pathology for their assistance in the selection of key images for this publication.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted June 11, 2011; Accepted June 22, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.6.6826
Address for Correspondence: Radhika Sundararajan, MD, PhD
Brigham and Women’s Hospital, Department of Emergency Medicine, 75 Francis St, Neville House 236A, Boston, MA 02115
E-mail: rsundararajan@partners.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding, sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Goldstein EB, Savel RH, Walter KL, et al. Extensive stage small cell lung cancer presenting as an acute perforated appendix: case report and review of the literature. Am Surg. 2004;70:706–709.[PubMed]
2. Wolf C, Friedl P, Obrist P, et al. Metastasis to the appendix: sonographic appearance and review of the literature. J Ultrasound Med. 1999;18:23–25. [PubMed]
3. Koff SG, Sterbis JR, Davison JM, et al. A unique presentation of appendicitis: F-18 FDG PET/CT.Clin Nucl Med. 2006;31:704–706. [PubMed]
4. Lu Y, Fox J, Dunphy M. Coincidental presentations of ganglioneuroma and atypical perforated appendicitis detected by fluorodeoxyglucose positron emission tomography/computed tomography. Clin Nucl Med. 2009;34:719–721. [PubMed]