
{kind=link}
| Author | Affiliation |
|---|---|
| Morgan Eutermoser, MD | Denver Health and University of Colorado Hospital, Department of Emergency Medicine, Denver, Colorado |
| Kristen Nordenholz, MD | Denver Health and University of Colorado Hospital, Department of Emergency Medicine, Denver, Colorado |
ABSTRACT
A 34-year-old male presented to the emergency department with a 3-hour complaint of pain in the right lower quadrant and right testicle. He stated that his pain began suddenly while standing at work. On physical examination, he had a small, firm, unreducible bulge in his right inguinal canal and an enlarged right scrotum. The patient was placed in trendelenburg position; intravenous fentanyl, valium, and dilaudid were administered; and surgery consult was obtained. A testicular ultrasonogram (Figure) was obtained owing to continued pain in the right scrotum and inability to evaluate the testicle. After viewing the ultrasound pattern, the patient was promptly taken to the operating room 6 hours after onset of symptoms.
INDIRECT INGUINAL HERNIA WITH TESTICULAR COMPROMISE
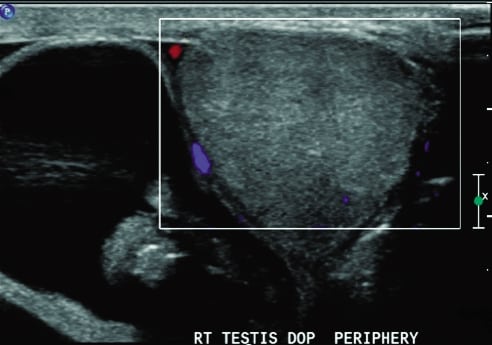
Testicular compromise is most commonly due to testicular torsion; however, this case highlights the risk to the testicle with an incarcerated inguinal hernia. In this patient, the physical examination yielded a bulge at the inguinal canal with diffuse scrotal enlargement, tenderness, and firmness. The patient’s testicle could not be evaluated, and therefore, ultrasonography was used to evaluate for concomitant torsion. The ultrasonogram revealed bowel inside the scrotal sac with no blood flow to the testicle due to compression of the spermatic cord. The spermatic cord contains 3 arteries, most notably the testicular artery, which experience reduced flow during torsion. Diagnosis of torsion can be confirmed by ultrasonography1 if examination is questionable.
Although testicular ischemia due to hernias has been well documented in pediatric literature, only 1 case report was found demonstrating this complication in the adult patient.2 The case report described a 48-year-old male who required only manual reduction to return flow to the testicle. If the mechanism of arterial compression is analogous to torsion, then the time to reduction and return of blood flow should be less than 6 hours to prevent permanent ischemia.3 Operative visualization of the testicle after hernia reduction revealed a normal testicle without evidence of ischemic change, and our patient was discharged shortly after the operation.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted May 25, 2011; Accepted July 21, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.7.6808
Address for Correspondence: Morgan Eutermoser, MD
Denver Health and University of Colorado Hospital, Department of Emergency Medicine, 777 Bannock St, Denver, CO 80204
E-mail: pinkstonmd@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding, sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Prando D. Torsion of the spermatic cord: the main gray-scale and doppler sonographic signs.Abdom Imaging. 2009;34:648–661. [PubMed]
2. Desai Y, Tollefson B, Mills L, et al. Testicular ischemia resulting from an inguinal hernia. J Emerg Med. [published online ahead of print September 10, 2010]
3. Kapoor S. Testicular torsion: a race against time. Int J Clin Pract. 2008;62:821–827. [PubMed]