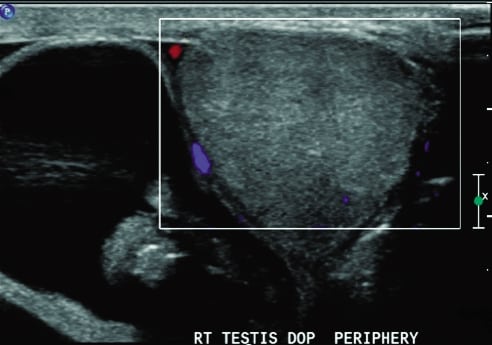
A 34-year-old male presented to the emergency department with a 3-hour complaint of pain in the right lower quadrant and right testicle. He stated that his pain began suddenly while standing at work. On physical examination, he had a small, firm, unreducible bulge in his right inguinal canal and an enlarged right scrotum. The patient was placed in trendelenburg position; intravenous fentanyl, valium, and dilaudid were administered; and surgery consult was obtained. A testicular ultrasonogram (Figure) was obtained owing to continued pain in the right scrotum and inability to evaluate the testicle. After viewing the ultrasound pattern, the patient was promptly taken to the operating room 6 hours after onset of symptoms.
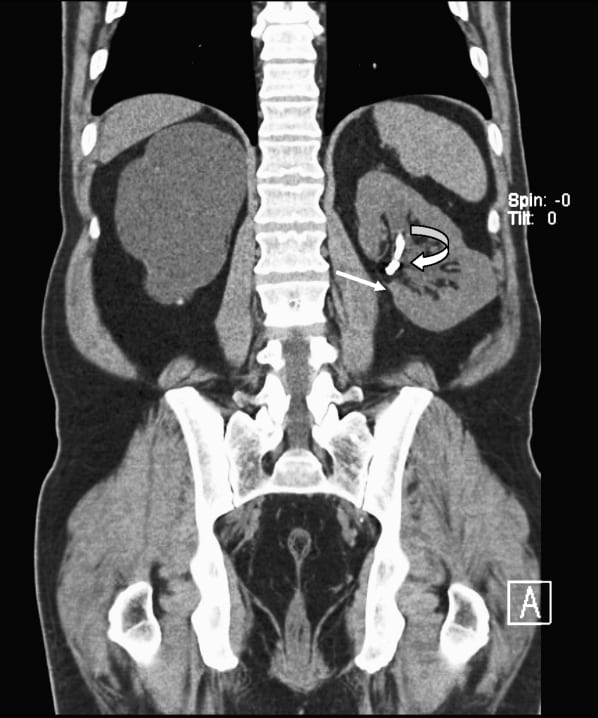
Urinary tract interventions can lead to multiple complications in the renal collecting system, including retained foreign bodies from endourologic or percutaneous procedures, such as stents, nephrostomy tubes, and others. We report a case of very delayed erosion of embolization coils migrating into the renal pelvis, acting as a nidus for stone formation, causing mild obstruction and finally leading to gross hematuria roughly 18 years post transarterial embolization. History is significant for a remote unsuccessful endopyelotomy attempt that required an urgent embolization.
In this report, we discuss a case of a 14-month-old male presenting in the emergency department with refusal to bear weight on his left leg. Plain radiographic studies revealed no evidence of effusion, fracture, or dislocation.
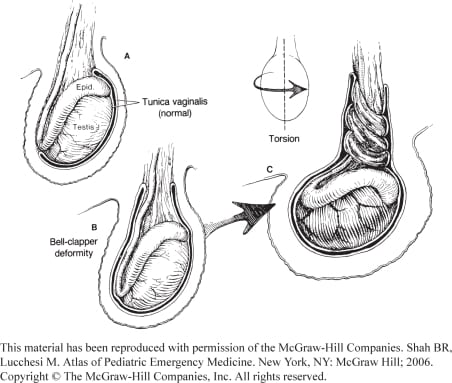
Although true urologic emergencies are extremely rare, they are a vital part of any emergency physician’s (EP) knowledge base, as delays in treatment lead to permanent damage. The four urologic emergencies discussed are priapism, paraphimosis, testicular torsion, and Fournier’s gangrene. An overview is given for each, including causes, pathophysiology, diagnosis, treatment, and new developments.
{kind=link}