
{kind=link}
| Author | Affiliation |
|---|---|
| Bridget A Sinnott, MD | Madigan Army Medical Center, Department of Emergency Medicine, Tacoma, Washington |
| Jared Strote, MD, MS | University of Washington Medical Center, Division of Emergency Medicine, Seattle, Washington |
A healthy 19-year-old male presented with complaints of right ankle pain. Twelve hours before, he had jumped off a skateboard, inverting and abrading his right ankle. He noted continued bleeding from the injury and difficulty bearing weight. He had a 1-cm puncture-type wound anterolateral to his lateral malleolus with oozing blood. There was a large hematoma and diffuse tenderness to palpation over the entire lateral malleolus. Sensation, pulses, and strength were intact and there was no joint laxity.
Ankle radiographs showed pneumarthrosis and air in the soft tissues of the leg (Figure, parts a and b). There were no fractures, and ankle alignment was preserved. Stress views showed no widening of the mortise. The orthopedic surgery team was consulted.
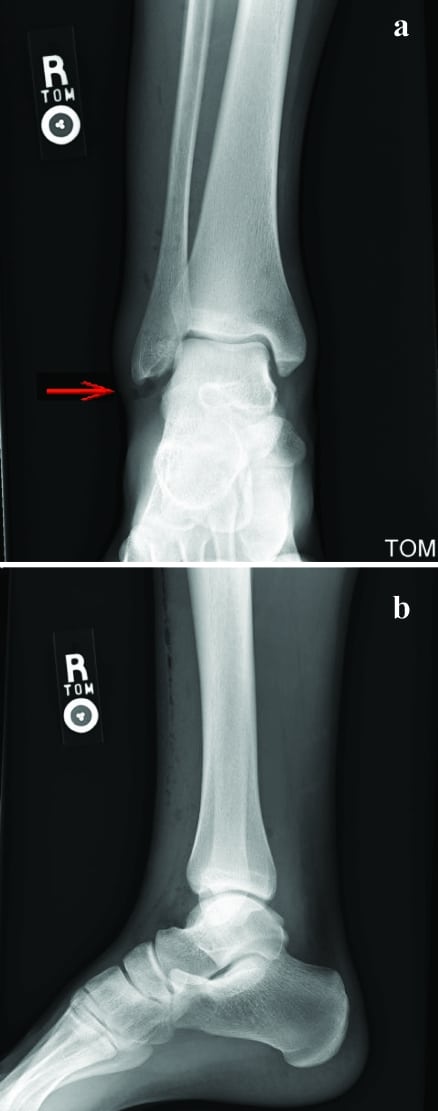
DIAGNOSIS: SEVERE OPEN ANKLE SPRAIN
The patient received cefazolin and underwent same-day ankle surgery. He was found to have an open ankle joint, which was irrigated. A tear across the anterolateral ligamentous complex was also repaired.
Severe open ankle sprain (SOAS) is a rare diagnosis, found in 0.2% of ankle injuries presenting to an orthopedic trauma center in the only study to date. It is associated with severe trauma such as motor vehicle accidents and falls from significant heights. Radiographic pneumarthrosis is seen in 56% of SOAS cases, and skin wounds are generally greater than 3 cm long.1 This patient’s low-velocity mechanism, lack of ankle laxity, and small wound suggested a diagnosis of stable ankle sprain with abrasion. Radiographic pneumarthrosis and intraoperative findings of severe ligamentous injury confirmed the diagnosis of SOAS.
It is important to differentiate SOAS from penetrating soft tissue injury, since treatment for SOAS is operative repair and antibiotics,1 whereas stable ankle sprains can be managed conservatively. In this case, radiographic evidence of air in the joint and soft tissue led to the diagnosis, despite a clinical presentation that differed from previous cases.
Footnotes
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Soubeyrand M, Vincent-Mansour C, Guidon J, et al. Severe open ankle sprain (SOAS): a lesion presenting as a penetrating soft tissue injury. J Foot Ankle Surg. 2010;;49:253–258. [PubMed]