
{kind=link}
| Author | Affiliation |
|---|---|
| Tara Hagopian, DO | Baylor College of Medicine, Department of Radiology, Houston, Texas |
| Fabricio Zuniga, MD | Corpus Christi Medical Center, Department of Family Practice, Corpus Christi, Texas |
| Salim R Surani, MD | Texas A&M University, Department of Medicine, Corpus Christi, Texas |
ABSTRACT
We present a case of pylephlebitis, which is an infective suppurative thrombosis of the portal vein. Pylephlebitis is an uncommon complication of intra-abdominal infections and carries with it significant morbidity and mortality.
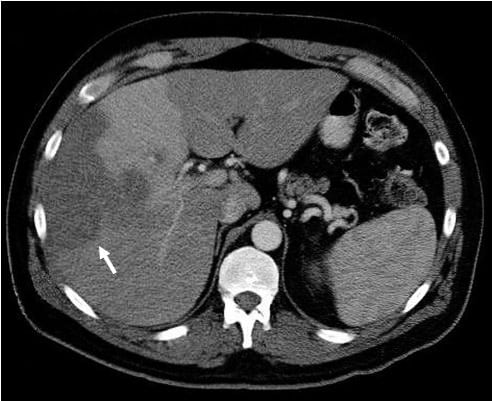
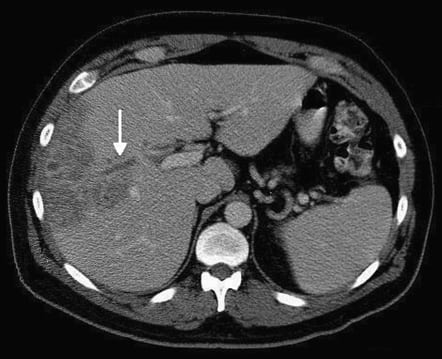
A 50-year-old Caucasian male with a history of asthma and a family history of venous thrombosis presented to the emergency department with the complaint of intermittent chest pain for 1 week, associated with progressive shortness of breath, fever, chills, nausea, and fatigue. The patient’s body temperature was 97.8°F; heart rate, 103/minute; respiratory rate, 32/minute; blood pressure, 111/65 mmHg; and oxygen saturation, 98% on room air. Physical examination was significant for diffuse abdominal tenderness, worse in the right upper quadrant. Laboratory examination revealed a white blood cell count of 24.2 K/mm3; aspartate aminotransferase, 43 IU/L; alanine aminotransferase, 64 IU/L; alkaline phosphatase, 299 IU/L; D-dimer, 5.01 mg/L; and Erythrocyte sedimentation rate, 119 MM/HR. Computed tomography (CT) results of the chest were negative for pulmonary embolus, and CT of the abdomen was performed (Figures 1 and 2). Imaging of the pelvis revealed sigmoid diverticulosis. Biopsy of the liver mass showed reactive and inflammatory changes consistent with abscess formation. Biopsy culture results, as well as blood culture results, were negative. Hypercoagulable workup revealed the presence of antiphospholipid antibodies. The patient showed clinical and radiologic improvement with appropriate antibiotic and anticoagulant therapy.
DIAGNOSIS
Pylephlebitis
Defined as infective suppurative thrombosis of the portal vein, pylephlebitis is an uncommon complication of intra-abdominal infections and carries with it significant morbidity and mortality. It occurs most commonly in association with diverticulitis and appendicitis, and in most cases more than 1 type of bacterial organism is found. The most common isolated microbes include Bacteroides,Enterococcus, Escherichia coli, Klebsiella, Staphylococcus, and Streptococcus.1 Treatment includes empiric therapy with broad-spectrum antibiotics, until cultures are available, with total treatment duration of 4 to 6 weeks.2
An associated hypercoagulable condition, malignancy, or acquired immune deficiency syndrome is not an uncommon finding.2 Anticoagulation therapy may reduce the incidence of septic embolization to the liver from infected portal thrombi and may prevent liver abscesses. The optimum duration of anticoagulation therapy is unclear.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted January 17, 2011; Accepted January 24, 2011
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2011.1.2197
Address for Correspondence: Salim Surani, MD
Texas A&M University, 613 Elizabeth St, Ste 813, Corpus Christi, TX 78413
E-mail: srsurani@hotmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Dugdale DC III, Vyas JM. Pyogenic liver abscess. MedlinePlus Web site. 2009. Available at:http://www.nlm.nih.gov/medlineplus/ency/article/000261.htm. Accessed June 1.
2. Spelman D. Pylephlebitis. UpToDate, Inc Web site. 2009. Available at:http://www.uptodate.com/online/content/topic.do?topicKey=gi_infec/7960&selectedTitle=1∼7&source=search_result. Accessed May 10.