As recent events highlight, a global requirement exists for evidence-based training in the emerging field of Disaster Medicine. The following is an example of an International Disaster Medical Sciences Fellowship created to fill this need. We provide here a program description, including educational goals and objectives and a model core curriculum based on current evidence-based literature. In addition, we describe the administrative process to establish the fellowship. Information about this innovative educational program is valuable to international Disaster Medicine scholars, as well as U.S. institutions seeking to establish formal training in Disaster Medical Sciences.
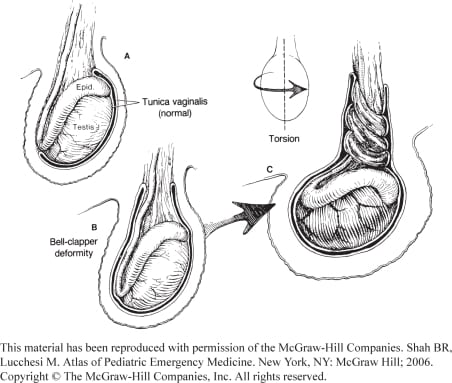
Although true urologic emergencies are extremely rare, they are a vital part of any emergency physician’s (EP) knowledge base, as delays in treatment lead to permanent damage. The four urologic emergencies discussed are priapism, paraphimosis, testicular torsion, and Fournier’s gangrene. An overview is given for each, including causes, pathophysiology, diagnosis, treatment, and new developments.
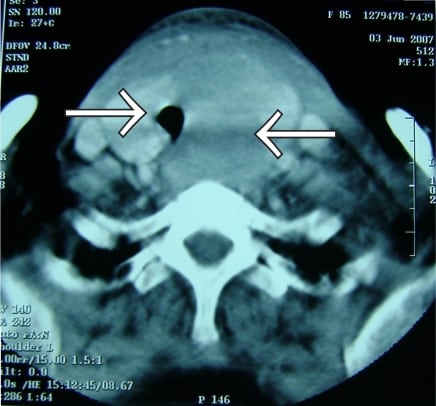
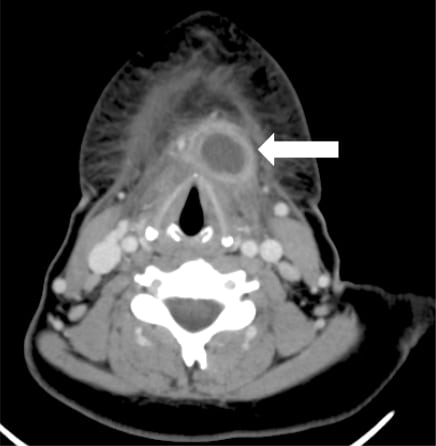
Hemorrhage of a previously normal thyroid gland as a result of blunt trauma is a very rare condition. We report a case of blunt trauma that caused acute hemorrhage into the thyroid gland and presented with hoarseness. The diagnosis of thyroid gland hematoma was made with a combination of fiberoptic laryngoscopy, cervical computed tomography, and carotid angiography. The patient was treated conservatively, had a favorable course without further complications, and was discharged four days after admission.
A 32-year-old man presented to the emergency department (ED) with lower abdominal pain and constipation. He related chronic ingestion of large amounts of opium. Physical examination showed mild abdominal tenderness and gingival discoloration. Diagnostic studies showed a mild hypochromic, microcytic anemia with basophilic stippling of the red blood cells. Abdominal imaging showed no intra-abdominal pathology. A diagnosis of lead toxicity was confirmed through serum lead levels. The patient was put on chelation therapy and his signs and symptoms started to resolve. As a comprehensive search for other sources of lead was unsuccessful, opium adulterants were considered as the culprit. Chemical analysis of the opium confirmed this. Contaminated drugs have been reported as a source of exposure to toxins such as arsenic or lead. While other reports deal with patients from clinics, this report illustrates lead toxicity from ingestion of contaminated opium in the ED.
A 15-year-old female presented to the emergency department with complaints of vaginal bleeding. She was pale, anxious, cool and clammy with tachycardic, thready peripheral pulses and hemoglobin of 2.4g/dL. Her abdomen was gravid appearing, approximately early to mid-second trimester in size. Pelvic examination revealed 2 cm open cervical os with spontaneous discharge of blood, clots and a copious amount of champagne-colored grapelike spongy material. After 2L boluses of normal saline and two units of crossmatched blood, patient was transported to the operating room. Surgical pathology confirmed a complete hydatidiform mole.
Emergency department (ED) crowding is a multifactorial problem, resulting in increased ED waiting times, decreased patient satisfaction and deleterious domino effects on the entire hospital. Although difficult to define and once limited to anecdotal evidence, crowding is receiving more attention as attempts are made to quantify the problem objectively.
The ability to perform drug calculations accurately is imperative to patient safety. Research into paramedics’ drug calculation abilities was first published in 2000 and for nurses’ abilities the research dates back to the late 1930s. Yet, there have been no studies investigating an undergraduate paramedic student’s ability to perform drug or basic mathematical calculations. The objective of this study was to review the literature and determine the ability of undergraduate and qualified paramedics to perform drug calculations.
Author Affiliation Mark I. Langdorf, MD, MHPE University of California, Irvine School of Medicine, Department of Emergency Medicine, Orange, CA Francesco Della Corte, MD University of Eastern Piedmont School of Medicine, Department of Anesthesia, Critical Care and Critical Emergency Medicine, Novara, Italy Roberta Petrino, MD St. Andrea Hospital, Department of Emergency Medicine, Vercelli, Italy […]
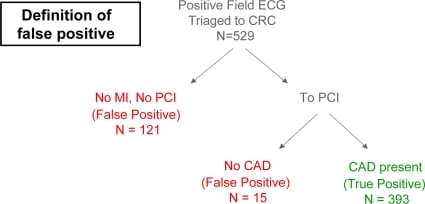
In 2005, Orange County California Emergency Medical Services (EMS) initiated a field 12-lead program to minimize time to emergency percutaneous coronary intervention (PCI) for field-identified acute myocardial infarction (MI). As the program matured, “false-positive” (defined as no PCI or coronary artery occlusion upon PCI) field MI activations have been identified as a problem for the program.
A 66-year-old man with a history of ankylosing spondylitis presented to the emergency department as a trauma activation after a fall backward onto his sacrum from the bottom rung of a ladder.
We sought to identify factors associated with need for mechanical ventilation (MV), length of intensive care unit (ICU) stay, length of hospital stay, and poor outcome in injection drug users (IDUs) with wound botulism (WB).
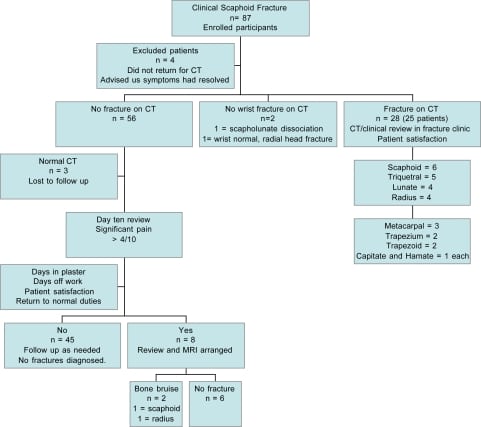
We developed and implemented clinical practice guideline (CPG) using computerized tomography (CT) as the initial imaging method in the emergency department management of scaphoid fractures. We hypothesized that this CPG would decrease unnecessary immobilization and lead to earlier return to work.
Author Affiliation Peter J. Bloomfied, MD, MPH Olive View-UCLA Medical Center, Department of Emergency Medicine, Sylmar, CA; Brotman Medical Center, Department of Emergency Medicine, Culver City, CA Adam B. Landman, MD, MS, MIS Robert Wood Johnson Foundation Clinical Scholars Program, Yale University School of Medicine, Department of Emergency Medicine, New Haven, CT; US Department […]
Author Affiliation William K. Mallon, MD Immediate Past-President, California Chapter of the American College of Emergency Physicians Stuart P. Swadron, MD Immediate Past-President, California Chapter of the American Academy of Emergency Medicine When you look at the Western Journal of Emergency Medicine’s (WestJEM) cover and masthead this month you will see something new: two logos […]
Author Affiliation Troy E. Madsen, MD University of Utah, Division of Emergency Medicine, Salt Lake City, UT Anne Bennett, MD University of Utah, Division of Emergency Medicine, Salt Lake City, UT Steven Groke, BSN University of Utah, Division of Emergency Medicine, Salt Lake City, UT Anne Zink, MD University of Utah, Division of Emergency […]
60-year-old Hispanic male with a history of smoking presented to the emergency department with complaint of dysphagia for the past two months. Additional symptoms included progressive shortness of breath and stridor.
While unsafe abortions have become rare in the United States, the practice persists. We present a 24-year-old female with a 21-week twin gestation who presented to the emergency department with complications of an attempted self-induced abortion. Her complicated clinical course included sepsis, chorioamnionitis, fetal demise, and a total abdominal hysterectomy with bilateral salpingo-oophorectomy for complications of endomyometritis. We discuss unsafe abortions, risk factors, and the management of septic abortion. Prompt recognition by the emergency physician and aggressive management of septic abortion is critical to decreasing maternal morbidity and mortality.
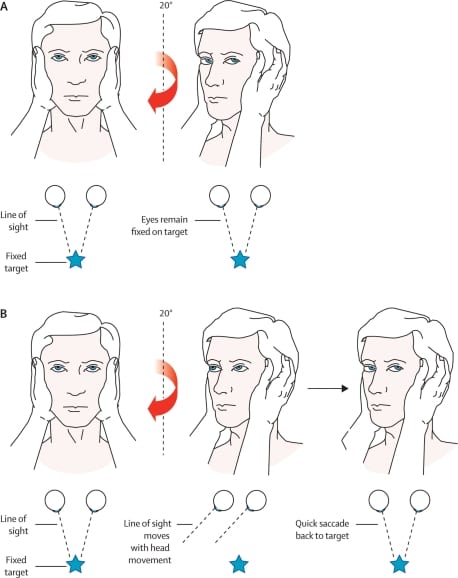
This article summarizes the emergency department approach to diagnosing cerebellar infarction in the patient presenting with vertigo. Vertigo is defined and identification of a vertigo syndrome is discussed. The differentiation of common vertigo syndromes such as benign paroxysmal positional vertigo, Meniere’s disease, migrainous vertigo, and vestibular neuritis is summarized. Confirmation of a peripheral vertigo syndrome substantially lowers the likelihood of cerebellar infarction, as do indicators of a peripheral disorder such as an abnormal head impulse test. Approximately 10% of patients with cerebellar infarction present with vertigo and no localizing neurologic deficits. The majority of these may have other signs of central vertigo, specifically direction-changing nystagmus and severe ataxia.
A 25-year-old healthy Hispanic male agricultural laborer presented to the emergency department with six weeks of a painless raised lesion on the proximal thumb with occasional drainage of fluid, without history of injury.
Many emergency department (ED) patients with cardiopulmonary symptoms such as chest pain or dyspnea are placed in observation units but do not undergo specific diagnostic testing for pulmonary embolism (PE). The role of observation units in the diagnosis of PE has not been studied. We hypothesized that there was a small but significant rate of unsuspected PE in our observation unit population.
A 17-year-old male presented to the emergency department with complaints of fever, rash that originated on the abdomen, malaise, and a cough for 10 days prior to evaluation.
A 23-year-old female presented to the emergency department (ED) with a five-day history of sore throat, body aches and 24 hours of throat swelling accompanied by globus sensation and hoarseness.
A previously healthy 31-year-old man presented to the emergency department complaining of right foot pain and a non-pruritic rash with swelling for one day.
{kind=link}