
{kind=link}
| Author | Affiliation |
|---|---|
| Alexander T. Limkakeng, Jr., MD | Duke University Medical Center, Division of Emergency Medicine, Durham, NC |
| Seth W. Glickman, MD | Duke University Medical Center, Division of Emergency Medicine, Durham, NC |
| Charles B. Cairns, MD | University of North Carolina at Chapel Hill, Department of Emergency Medicine |
| Abhinav Chandra, MD | Duke University Medical Center, Division of Emergency Medicine, Durham, NC |
ABSTRACT
Introduction:
Many emergency department (ED) patients with cardiopulmonary symptoms such as chest pain or dyspnea are placed in observation units but do not undergo specific diagnostic testing for pulmonary embolism (PE). The role of observation units in the diagnosis of PE has not been studied. We hypothesized that there was a small but significant rate of unsuspected PE in our observation unit population.
Methods:
We performed a retrospective chart review at an urban academic hospital of all ED patients with an International Classification of Diseases, Ninth Revision diagnosis of PE between January 2005 and July 2006. The number of such patients assigned to observation at any point in their stay was recorded, in addition to events leading to diagnosis and subsequent in-hospital outcomes.
Results:
Thirteen of the 190 ED patients diagnosed with PE were placed in the observation unit. Six of these either had a known recent diagnosis of PE or had testing for PE initiated prior to placement in the observation unit. Two of the remaining seven patients with undiagnosed PE were placed in observation for undifferentiated chest pain, accounting for 0.09% of the 2190 patients under the chest pain protocol. Twelve of 13 PE patients (92%) were admitted with an average stay of 4.3 days. Of the 13 patients, five were ultimately determined after admission to not have PE, leaving a rate of confirmed PE in the observation unit population of 0.12% (8/6182), with five of eight being classified as unsuspected prior to assignment to observation (0.08% rate).
Conclusion:
We identified a small number of patients assigned to observation with unsuspected PE. The high rate of hospital admission and prolonged hospital stay suggests that patients with PE are inappropriate for observation status. Given the low incidence of unsuspected PE, there may be a need for a specific approach to screening for PE in observation unit patients.
INTRODUCTION
Evaluation for acute coronary syndrome accounts for over five million emergency department (ED) visits.1–6 Observation units have been demonstrated to reduce costs and increase efficiency for symptoms suggestive of acute coronary syndrome and thus have become widespread.7–14 While the differential diagnosis for such symptoms also includes pulmonary embolism (PE), many patients do not receive formal evaluation for PE.
PE is a potentially fatal condition with a wide variety of presentations. Many of these overlap symptoms for which patients are placed in observation.15–21 It has been demonstrated that the risk of mortality from PE can be reduced by early diagnosis.22–25Therefore, determining which patients need diagnostic evaluation prior to placement in an observation unit remains an important challenge for emergency physicians (EP). Placing patients with undiagnosed PE in observation could lead to preventable morbidity and even mortality. Despite anecdotes of patients with unsuspected PE being assigned to observation units, to our knowledge the rate of PE in this population has not been reported.
We sought to determine the rate of unsuspected PE diagnosed in the observation unit. We hypothesized that the rate of patients being diagnosed with unsuspected PE while under observation is significant. If so, routine diagnostic testing might be considered prior to placement in an observation unit. Additionally, if such PE patients were found to have short hospital courses, observation unit protocols could be developed to facilitate their care.
METHODS
We performed a retrospective chart review of all patients with an International Classification of Diseases, Ninth Revision (ICD-9) diagnosis of PE seen in the ED of an urban academic medical center between January 2005 and July 2006. During this time period our observation unit had no standardized approach to the evaluation of PE. Thus, all diagnoses of PE made there were made based on changes in patient condition or a re-evaluation. Using a hospital billing database, we identified 190 patients with primary or secondary ICD-9 diagnosis of PE, who accounted for 209 ED visits. Two reviewers independently ascertained from each electronic chart whether or not the patient had been assigned to the observation unit at any point in the ED visit, as well as what their diagnoses were on discharge from the hospital. Given the low number of patients and relatively simple data point measurement, we determined no need for reviewer training or monitoring. Reviewers had 100% agreement that all patients identified were indeed placed in the observation unit. We noted relevant clinical data such as reason for observation, method by which patient was diagnosed with PE, need for hospital admission, and length of stay. Wells criteria were noted with the exception of whether there was an alternative diagnosis more likely than PE, as this could not always be ascertained from the chart. We also recorded any adverse outcomes, such as intensive care unit admission, intubation, need for vasopressors, and death. This study met criteria for exemption from local institutional review committee.
We sub-categorized some patients with PE diagnoses as being unsuspected and some as confirmed. We considered a PE to be unsuspected if no laboratory testing such as D-dimer or radiology diagnostic testing, such as ventilation perfusion scan, computed tomography angiogram of the chest, or pulmonary angiography, was ordered prior to observation unit assignment. A patient had a confirmed PE if this was their discharge diagnosis. We used simple proportions with 95% confidence intervals.
RESULTS
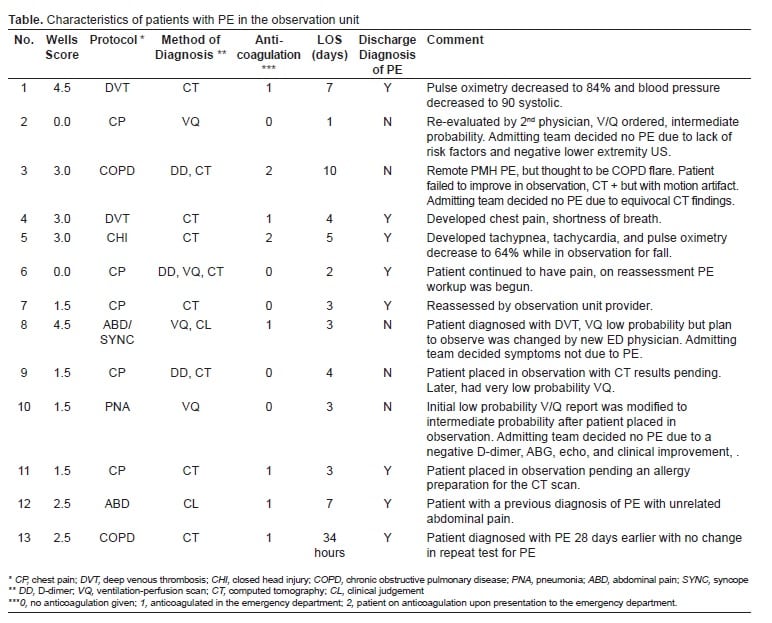
Thirteen of the 190 (7%) ED patients diagnosed with PE were placed in the observation unit (Figure). Twelve of 13 PE patients (92%) were admitted with an average length of stay of 4.3 days. None of the patients died, required intensive care unit admission, or invasive interventions for complications.
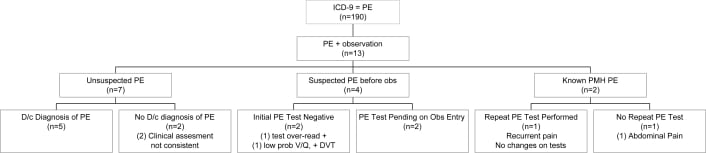
Eleven of 13 patients (85%) had not been diagnosed with PE prior to observation unit. Of these, seven patients did not have any testing for PE prior to observation and were classified as unsuspected. Five (38%) of the 13 patients were discharged without the diagnosis of PE despite the initial ED ICD-9 code (Table). The inpatient team’s evaluation of these patients was thought to be inconsistent with PE, despite suggestive testing in the ED.
During this time 6,182 patients were placed in observation. Including only the eight with a confirmed PE at hospital discharge, we found a 0.12% rate (8/6182, 95% CI 0.03–0.20%) of PE diagnosed in our observation unit. Since three of these had PE testing initiated prior to observation, we calculate a 0.08% rate (5/6182, 95% CI 0.01–0.15%) of unsuspected, confirmed PE.
Two were placed in observation for chest pain, leaving a diagnosis rate of 0.09% in 2,190 chest pain patients. By comparison, 14% of chest pain patients ruled in for acute coronary syndrome (ACS). Two with unsuspected PE were entered under the deep venous thrombosis (DVT) protocol and one under the chronic obstructive pulmonary disease (COPD) protocol representing 2.7% (2/73) and 1.0% (1/97), respectively, of the patients under these observation protocols.
DISCUSSION
Given the low rate of coronary disease in observation unit patients, it is possible that other etiologies are responsible for their symptoms. One such possibility is PE. It has been recently demonstrated that patients with PE diagnosed in the ED have fewer complications than those in whom the diagnosis is delayed.25 Therefore, such patients in the observation unit may be at significant risk for a preventable poor outcome.
To our knowledge, this is the first report on the rate of PE diagnosed in an ED observation unit. A previous multicenter prospective effort failed to identify any patients placed in the observation unit for chest pain with subsequent diagnosis of PE or aortic dissection.26Other authors have reported on significant adverse events in the observation unit. Mace reviewed all observation unit patients requiring resuscitation over a 25- month time period. Of 10,245 patients, only nine (0.09%) required resuscitation as defined by chest compressions, defibrillation, assisted ventilation, or advanced cardiac life support medications. None of these nine were reported to have PE as the cause of their decompensation.27 In a large Taiwanese study of 7,028 observation unit patients over six months, 175 initially stable patients decompensated to critical conditions requiring resuscitation. The critical conditions identified included respiratory distress, apnea, shock, dysrhythmia, gastrointestinal bleeding, altered mental status and seizure. None of them were noted to have PE identified as the cause of their decompensation.28
It is worth noting that the few patients in our study with unsuspected PE were diagnosed due to changes in clinical condition or re-evaluation by another clinician. This highlights the difficulty in diagnosis. Previous research has sought to define an ideal algorithmic approach.15, 29–39 Although it was not specifically designed to address this question, our findings suggest that routine D-dimer screening prior to observation unit assignment would be a low-yield strategy. Furthermore, the rate of clinical risk factors in our low-risk observation unit population is lower than what might be expected. Thus, the standard clinical stratification systems may not be as valuable in these patients. Complicating matters further, a number of our patients diagnosed with PE by objective testing in the ED were judged to not have PE on further workup in an inpatient setting. This demonstrates even further the often subjective nature of this diagnosis.
Given that DVT and PE share a similar pathophysiology it is not surprising to find patients in our DVT protocol developing PE. One interesting finding was the percentage of patients in the COPD protocol with PE. Previous authors who have attempted to identify whether the presence of COPD obscures the diagnosis of PE found a similar rate of PE and similar pre-test characteristics compared to patients without COPD.40 Although our data is limited by a relatively low event rate, the relatively high proportion of patients with primary symptoms other than chest pain reflects the diversity of presentations of PE and again suggests that EPs keep a high level of vigilance.
Recent data has suggested that even PE with less severe clinical symptoms is associated with worse outcomes with delayed diagnosis.25 Therefore, even PE patients with a subclinical initial course might still be at risk. None of the observation unit patients in our study with initially undiagnosed PE died or had a serious adverse outcome. However, most were hospitalized with a prolonged average length of stay. Therefore, it is arguable whether these cases should be viewed as an unheralded benefit of observation (the prolonged observation period made the diagnosis possible) or narrowly averted mistakes in patient management. In either case, our findings suggest the need for continued reassessment of patients under observation status. Observation unit staffing models need to accommodate this need.
LIMITATIONS
We don’t know how many patients had diagnostic workup for PE before being assigned to observation during this time period. In a separate analysis of a different set of chest pain observation patients at this center, 21% had diagnostic workup for PE before being assigned to observation. Thus, it is likely that a significant portion of the observation unit patients in this study had already had an evaluation for PE, making the likelihood of finding those with unsuspected PE even less.
Our study was also limited by its retrospective methodology. Our results are thus dependent on the accuracy of the ICD-9 data. Furthermore, only patients diagnosed in the ED were included. Because we do not have follow-up on the many patients evaluated in our observation unit it is possible that there were some PE patients diagnosed after observation unit evaluation or diagnosed on a subsequent ED visit. Thus, there may have been patients with PE who are not captured in this study. Our data do not allow us to calculate a true incidence of unsuspected PE in the observation unit, merely the rate at which the diagnosis was made.
Furthermore, we did not catalog the diagnostic testing of patients admitted from observation after being diagnosed with PE. Thus, we cannot comment on the appropriateness of such admissions, whether the length of stay was appropriate, or whether such patients truly could have remained in an observation unit setting.
CONCLUSION
We identified a small but significant number of observation unit patients with unsuspected PE. This rate appears low enough that routine diagnostic screening would not likely be of benefit. Because these patients are not easily characterized, EPs need to be vigilant for the diagnosis prior to observation unit assignment. This study also highlights the need for adequate staffing and re-evaluation of observation patients. Future research should focus on developing better ways to identify which should have diagnostic testing prior to observation unit assignment, or incorporate such testing within the observation unit protocol.
Footnotes
Supervising Section Editor: Jeffrey Sankoff, MD
Submission history: Submitted July 17, 2008; Revision Received November 03, 2009; Accepted November 09, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Alexander T. Limkakeng, Jr., MD, Department of Surgery, Duke University Medical Center, Division of Emergency Medicine, DUMC Box 3096, Durham, NC 27710
Email: alexander.limkakeng@duke.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Thom T, Haase N, Rosamond W, et al. Heart disease and stroke statistics–2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113:e85–151. [PubMed]
2. Nawar EW, Niska RW, Xu J. National hospital ambulatory medical care survey: 2005 emergency department summary. Adv Data. 2007;386:1–32. [PubMed]
3. Swap CJ, Nagurney JT. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA. 2005;294:2623–2629.[PubMed]
4. Limkakeng A, Jr, Gibler WB, Pollack C, et al. Combination of Goldman risk and initial cardiac troponin I for emergency department chest pain patient risk stratification. Acad Emerg Med. 2001;8:696–702. [PubMed]
5. Pope JH, Selker HP. Acute coronary syndromes in the emergency department: Diagnostic characteristics, tests, and challenges. Cardiol Clin. 2005;23:423–51. v–vi.[PubMed]
6. Pope JH, Ruthazer R, Beshansky JR, et al. Clinical features of emergency department patients presenting with symptoms suggestive of acute cardiac ischemia: A multicenter study. J Thromb Thrombolysis. 1998;6:63–74. [PubMed]
7. Goodacre S, Nicholl J, Dixon S, Cross E, Angelini K, Arnold J, Revill S, Locker T, Capewell SJ, Quinney D, Campbell S, Morris F. Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care. BMJ.2004;328:254. [PMC free article] [PubMed]
8. Rydman RJ, Zalenski RJ, Roberts RR, et al. Patient satisfaction with an emergency department chest pain observation unit. Ann Emerg Med. 1997;29:109–15. [PubMed]
9. Taubenhaus KJ, Robilotti GD. The holding area: New arm of the emergency department. JACEP. 1972;1:15–19.
10. Bobzien WF., 3rd The observation-holding area; a prospective study. JACEP.1979;8:508–12. [PubMed]
11. Wilkinson K, Severance H. Identification of chest pain patients appropriate for an emergency department observation unit. Emerg Med Clin North Am. 2001;19:35–66.[PubMed]
12. Landers GA, Waeckerle JF, McNabney WK. Observation ward utilization. JACEP.1975;4:123–25.
13. Kelen GD, Scheulen JJ, Hill PM. Effect of an emergency department (ED) managed acute care unit on ED overcrowding and emergency medical services diversion. Acad Emerg Med. 2001;8:1095–100. [PubMed]
14. Goodacre S, Locker T, Arnold J, et al. Which diagnostic tests are most useful in a chest pain unit protocol? BMC Emerg Med. 2005;5:6. [PMC free article] [PubMed]
15. American College of Emergency Physicians Clinical Policies Committee, Clinical Policies Committee Subcommittee on Suspected Pulmonary Embolism Clinical policy: Critical issues in the evaluation and management of adult patients presenting with suspected pulmonary embolism. Ann Emerg Med. 2003;41:257–70. [PubMed]
16. PISAPED Investigators Invasive and noninvasive diagnosis of pulmonary embolism. preliminary results of the prospective investigative study of acute pulmonary embolism diagnosis (PISA-PED) Chest. 1995;107(1 Suppl):33S–38S. [PubMed]
17. Kokturk N, Oguzulgen IK, Demir N, et al. Differences in clinical presentation of pulmonary embolism in older vs younger patients. Circ J. 2005;69:981–86. [PubMed]
18. Pineda LA, Hathwar VS, Grant BJ. Clinical suspicion of fatal pulmonary embolism.Chest. 2001;120:791–5. [PubMed]
19. Stein PD, Henry JW. Clinical characteristics of patients with acute pulmonary embolism stratified according to their presenting syndromes. Chest. 1997;112:974–9.[PubMed]
20. Stein PD, Henry JW. Prevalence of acute pulmonary embolism among patients in a general hospital and at autopsy. Chest. 1995;108:978–981. [PubMed]
21. Kabrhel C, Camargo CA, Jr, Goldhaber SZ. Clinical gestalt and the diagnosis of pulmonary embolism: Does experience matter? Chest. 2005;127:1627–30. [PubMed]
22. Brown MD, Vance SJ, Kline JA. An emergency department guideline for the diagnosis of pulmonary embolism: An outcome study. Acad Emerg Med. 2005;12:20–5. [PubMed]
23. Kline JA, Webb WB, Jones AE, et al. Impact of a rapid rule-out protocol for pulmonary embolism on the rate of screening, missed cases, and pulmonary vascular imaging in an urban US emergency department. Ann Emerg Med. 2004;44:490–502. [PubMed]
24. Calder KK, Herbert M, Henderson SO. The mortality of untreated pulmonary embolism in emergency department patients. Ann Emerg Med. 2005;45:302–10.[PubMed]
25. Kline JA, Hernandez-Nino J, Jones AE, et al. Prospective study of the clinical features and outcomes of emergency department patients with delayed diagnosis of pulmonary embolism. Acad Emerg Med. 2007;14:592–8. [PubMed]
26. Chandra A, Chiumento AB, Benjamin L, et al. Lack of pulmonary embolism and aortic dissection in chest pain patients evaluated in a chest pain observation unit. Ann Emerg Med. 2006;48:89–90.
27. Mace SE. Resuscitations in an observation unit. J Qual Clin Pract. 1999;19:155–64.[PubMed]
28. Chang Y, Chen C, Chang C, et al. Evaluation of unpredictable critical conditions of patients treated in the observation unit of the emergency department. J Emerg Med.2004;27:109–113. [PubMed]
29. Brown MD, Rowe BH, Reeves MJ, et al. The accuracy of the enzyme-linked immunosorbent assay D-dimer test in the diagnosis of pulmonary embolism: A meta-analysis. Ann Emerg Med. 2002;40:133–144. [PubMed]
30. Caine GJ, Lip GY. Validity of D-dimer tests for pulmonary embolism: Better to diagnose or exclude? Ann Emerg Med 2003. 41756author reply 756–7. [PubMed]
31. Dunn KL, Wolf JP, Dorfman DM, et al. Normal D-dimer levels in emergency department patients suspected of acute pulmonary embolism. J Am Coll Cardiol.2002;40:1475–78. [PubMed]
32. Farrell S, Hayes T, Shaw M. A negative SimpliRED D-dimer assay result does not exclude the diagnosis of deep vein thrombosis or pulmonary embolus in emergency department patients. Ann Emerg Med. 2000;35(2):121–5. [PubMed]
33. Ghanima W, Almaas V, Aballi S, et al. Management of suspected pulmonary embolism (PE) by D-dimer and multi-slice computed tomography in outpatients: An outcome study. J Thromb Haemost. 2005;3:1926–1932. [PubMed]
34. Goldstein NM, Kollef MH, Ward S, et al. The impact of the introduction of a rapid D-dimer assay on the diagnostic evaluation of suspected pulmonary embolism. Arch Intern Med. 2001;161:567–571. [PubMed]
35. Kabrhel C, Matts C, McNamara M, et al. A highly sensitive ELISA D-dimer increases testing but not diagnosis of pulmonary embolism. Acad Emerg Med. 2006;13:519–524.[PubMed]
36. Kearon C, Ginsberg JS, Douketis J, et al. An evaluation of D-dimer in the diagnosis of pulmonary embolism: a randomized trial. Ann Intern Med. 2006;144:812–821.[PubMed]
37. Kline JA, Nelson RD, Jackson RE, et al. Criteria for the safe use of D-dimer testing in emergency department patients with suspected pulmonary embolism: A multicenter US study. Ann Emerg Med. 2002;39:144–152. [PubMed]
38. Kline JA, Runyon MS, Webb WB, et al. Prospective study of the diagnostic accuracy of the simplify D-dimer assay for pulmonary embolism in emergency department patients.Chest. 2006;129:1417–1423. [PubMed]
39. Stein PD, Woodard PK, Weg JG, et al. Diagnostic pathways in acute pulmonary embolism: Recommendations of the PIOPED II investigators. Radiology. 2007;242:15–21.[PubMed]
40. Hartmann IJ, Hagen PJ, Melissant CF, et al. Diagnosing acute pulmonary embolism: Effect of chronic obstructive pulmonary disease on the performance of D-dimer testing, ventilation/perfusion scintigraphy, spiral computed tomographic angiography, and conventional angiography. ANTELOPE study group. Advances in new technologies evaluating the localization of pulmonary embolism. Am J Respir Crit Care Med.2000;162:2232–37. [PubMed]