
{kind=link}
| Author | Affiliation |
|---|---|
| Laura Andrews | Keck School of Medicine of the University of Southern California, Department of Emergency Medicine, Los Angeles, CA |
| Sean O. Henderson, MD | Keck School of Medicine of the University of Southern California, Department of Emergency Medicine, Los Angeles, CA |
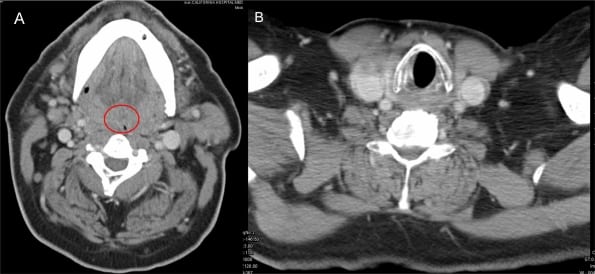
A 60-year-old Hispanic male with a history of smoking presented to the emergency department with complaint of dysphagia for the past two months. Additional symptoms included progressive shortness of breath and stridor. CT results from an outside institution showed 80% airway obstruction. Despite the findings, the patient’s vitals were normal, with respirations of 20 and an initial room air oxygen saturation of 98%. Palpable neck masses or lymphadenopathy were not noted at the time of physical exam. A CT revealed the absence of a visible airway (Figure 1a; compare with Figure 1b taken below the level of the mass) and an expansive soft-tissue mass roughly spanning spinal cord levels C1 to C6 (Figure 2). An emergent ENT consult was called and the patient was given dexamethasone to control edema and prevent further obstruction. He was taken to the operating room where he could not be intubated and underwent an emergency tracheotomy. Direct laryngoscopy and biopsy revealed significant epiglottic destruction by squamous cell carcinoma, with lymphangitic metastasis to the cervical soft tissues. Patient was given dexamethasone to control edema and prevent further obstruction.

Squamous cell carcinoma of the larynx occurs up to 30 times more frequently in men and is associated with a history of smoking and alcohol consumption, which together can increase the risk of laryngeal cancer by a factor greater than 100.1,2,3 Compared to glottic, supraglottic tumors have greater risk of lymphogenous metastasis due to greater vascularity and later presentation due to fewer symptoms.4 As a result, many patients presenting with advanced disease have palpable neck metastases.
The extensive obstruction that this patient presented with warrants mention of the management options available in such a case. The emergency physician needs to be aware of alternatives for salvaging the airway in these rare instances. The standard landmark-based cricothyrotomy would have been ineffective as the tumor obstructed this region entirely. While jet ventilation below the level of the obstruction could have been used as a temporizing measure, the only practical approach to establishing a definitive airway would have been to move the “cric” down several rings to a level free of obstruction.
Footnotes
Supervising Section Editor: Matthew Strehlow, MD
Submission history: Submitted June 26, 2008; Revision Received December 10, 2009; Accepted January 10, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Sean O. Henderson, MD, Department of Emergency Medicine, LAC+USC Medical Center, Unit #1, Room 1011, 1200 N. State Street, Los Angeles, CA 90033
Email: sohender@hsc.usc.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Hoffman HT, Porter K, Karnell LH, et al. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116:1–13. [PubMed]
2. Gronbaek M, Becker U, Johansen D, et al. Population based cohort study of the association between alcohol intake and cancer of the upper digestive tract. British Medical Journal.1998;317:844–47. [PMC free article] [PubMed]
3. Cosetti M, Yu GP, Schantz SP. Five-year survival rates and time trends of laryngeal cancer in the US population. Archives of Otolaryngology–Head & Neck Surgery. 2008;134:370–79. [PubMed]
4. Raitiola H, Pukander J, Laippala P. Glottic and supraglottic laryngeal carcinoma: differences in epidemiology, clinical characteristics and prognosis. Acta Oto-Laryngologica. 1999;119:847–51.[PubMed]