
{kind=link}
| Author | Affiliation |
|---|---|
| Baris Saylam, MD | Ankara Numune Teaching and Research Hospital, Department of 3rd Surgery, Ankara, Turkey |
| Bülent Çomçali, MD | Ankara Numune Teaching and Research Hospital, Department of 3rd Surgery, Ankara, Turkey |
| Mehmet Vasfi Ozer, MD | Ankara Numune Teaching and Research Hospital, Department of 3rd Surgery, Ankara, Turkey |
| Faruk Coskun, MD | Ankara Numune Teaching and Research Hospital, Department of 3rd Surgery, Ankara, Turkey |
ABSTRACT
Hemorrhage of a previously normal thyroid gland as a result of blunt trauma is a very rare condition. We report a case of blunt trauma that caused acute hemorrhage into the thyroid gland and presented with hoarseness. The diagnosis of thyroid gland hematoma was made with a combination of fiberoptic laryngoscopy, cervical computed tomography, and carotid angiography. The patient was treated conservatively, had a favorable course without further complications, and was discharged four days after admission.
INTRODUCTION
Trauma to the thyroid gland following blunt neck trauma is rarely reported in the English-language literature.1–15 Blunt direct thyroid injury is quite rare in trauma patients without preexisting goiter.1 Most of the reported cases have emphasized the need to closely monitor patients with thyroid injuries so that possible upper airway obstruction caused by an associated hematoma can be detected promptly.1,2,3,12
In all cases of blunt trauma involving the neck, a high index of suspicion is warranted as symptoms may not be present on initial examination. We report a case of blunt injury to a previously normal thyroid in which invasive airway management was not necessary and successful non-operative treatment was accomplished.
CASE REPORT
The patient, a 69-year-old female, fell in the bathroom on a slippery floor and struck her anterior neck. About three hours after the event, she was admitted by ambulance to the emergency department (ED) of our hospital. On admission, she was conscious and did not appear unduly distressed. There were no signs of emphysema, stridor or dyspnea. Her breath sounds were equal. The patient didn’t suffer any kind of aspiration or cough. Her vital signs were normal, showing a blood pressure of 130/80 mmHg, a heart rate of 66 bpm and a respiratory rate of 20 breaths per minute. Her arterial blood gas was normal, with an O2 saturation of 98% on room air. Although the vital signs were stable and she was not in respiratory distress, her voice was hoarse immediately following the injury. The patient was only able to speak in a whisper. On examination, her neck was swollen and was tender to palpation. No carotid bruits were auscultated. Plain films of the neck revealed a normal cervical spine with mild tracheal deviation toward the right. Because of the suspicion of a muscular hematoma, the patient underwent a sonographic examination of the neck. The neck ultrasound revealed a moderately hypoechoic, diffuse, infiltrative process presumed to be a hematoma surrounding the left thyroid lobe and extending into the anterior cervical muscular strap.
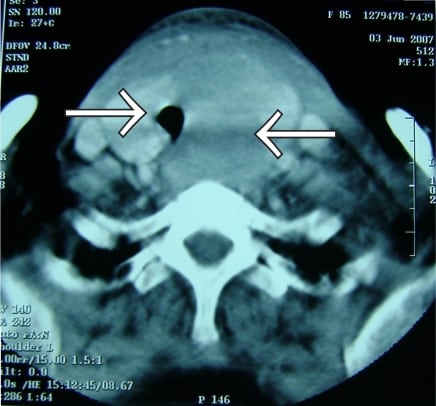
Computed tomography (CT) scan without contrast was performed to better evaluate the extent of the hematoma and the possible compromise of neighboring structures. However, neck CT scan demonstrated fragmentation and hematoma within the left lobe of the thyroid gland (Figure 1), as well as tracheal deviation to the right without evidence for laryngotracheal trauma. This study revealed a mass, felt to be a hematoma, in the left neck, measuring 4.7 × 5 × 5 cms. The left lobe of the thyroid was indistinguishable from the hematoma, and luminal narrowing was noted in the lower neck. A thyroid functional profile showed a moderate thyroid hormone disorder: free thyroxine, 1.05 pg/ml (reference range, 0.70–1.48 ng/dL), free triiodothyronine, 3.95 pg/mL (reference range, 1.71–3.71 pg/mL), and thyrotropin, 1.78 uIU/mL (reference range, 0.35–4.94uIU/mL). Hematologic analysis showed a WBC of 14 K/uL (normal: 4,4 to 11,3), with no other significant abnormalities.
Because the patient was hemodynamically stable with excellent oxygen saturations upon examination in the ED, further evaluation by means of cervical angiography and indirect laryngoscopy were planned. No signs of active bleeding or expanding hematoma were noted; however, cervical angiography was performed to rule out vascular injury. No vascular injury was found. Otolaryngology was consulted to perform indirect laryngoscopy for evaluation of possible laryngeal injury. Fiberoptic laryngoscopy performed by the consulting otolaryngologist revealed a patent supralaryngeal airway with ecchymoses and mild bilateral vocal-cord edema with an otherwise normal airway.
The patient was admitted to the surgical intensive care unit for close airway observation, reverse Trendelenberg and monitoring for progression of her neck hematoma. Over the ensuing four days, the size of the patient’s neck hematoma remained stable, no stridor or respiratory distress developed, and the patient’s voice weakness resolved. Follow-up sonography performed two months later showed a normal left thyroid lobe.
DISCUSSION
While blunt neck trauma is relatively common, secondary thyroid hemorrhage of a previously normal thyroid gland as a result of trauma is a very rare condition.2–7 Most of the reported cases affected a goitrous gland, with resultant increased size and vascularity increasing risk for hemorrhage.5,8,9,10,11 In our patient there was no history of goiter, thyroid gland adenoma, or hyperthyroidism.
Several circumstances have been associated with hemorrhage of the thyroid gland: trauma, deceleration injury, cervical hyperflexion, and Valsalva maneuvers that increase venous pressure, including straining during defecation or heavy lifting.5,9,10 Direct impact to the anterior neck as a result of blunt trauma has been associated with vascular, bony, muscular, laryngeal, tracheal, and esophageal injury. Onset of life-threatening symptoms in previous reports ranges from within 60 minutes5 to greater than 24 hours.8,10 Symptoms in cases of blunt thyroid trauma are similar to those in laryngotracheal trauma, with palpable painful, pretracheal or paratracheal neck mass. Other symptoms suggestive of possible thyroid trauma include respiratory compromise,5,10,12dysphagia,2.13 or hoarseness.1,2,5,14
Because of the rarity of blunt trauma to the thyroid gland, no consensus has emerged as to itsworkup or management. The diagnosis of isolated thyroid gland injury due to blunt neck trauma is difficult. Most of the reported patients are operated on urgently, and neck exploration confirms the diagnosis of thyroid gland injury.1,3,5,8,9,10
Emergency investigations, such as CT scan and/or ultrasonography of the neck, can establish the diagnosis of thyroid gland injury preoperatively. CT confirmed the thyroid gland rupture and surrounding hematoma, facilitating the evaluation of the larynx and the upper digestive tract. Transient hyperthyroidism15 and thyroid storm7 have been reported after a traumatic hemorrhage into a previously normal thyroid gland. Although thyroid hormone levels in our patient were borderline high immediately after the trauma, subsequently they were normal.
Fiberoptic laryngoscopy is also helpful to rule out laryngotracheal injury, as it is not always obvious on CT scans.2 In cases of blunt neck trauma with massive swelling, the most common injury is major vessel rupture. If this is suspected, then arterial angiography should be obtained.12
Initially, most cases of traumatic hemorrhage into the thyroid gland were treated with surgical evacuation and debridement. More recently, several cases of conservative management of thyroid hematomas have been published in the literature.2,3,4,6,14
CONCLUSION
We believe that in the acute setting, a stable thyroid hematoma without airway compromise may be safely observed. Potential airway encroachment is the main endication for neck exploration.
Footnotes
Supervising Section Editor: Teresita M. Hogan, MD
Submission history: Submitted May 20, 2009; Revision Received October 2, 2009; Accepted October 12, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Faruk Coskun, Associate Professor of Surgery, Director of 3rd Surgery Department, Ankara Numune Teaching and Research Hospital, Department of 3rd Surgery, Sehit Adem Yavuz Sokak No: 7/11, 06100-Kizilay, Ankara, Turkey
Email: mdbsaylam@yahoo.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Heizmann O, Schmid R, Oertli D. Blunt injury to the thyroid gland: Proposed classification and treatment algorithm. J Trauma. 2006;61:1012–5. [PubMed]
2. Weeks C, Moore FD, Ferzoco SJ, et al. Blunt trauma to the thyroid: a case report. Am Surg.2005;71:518–20. [PubMed]
3. Hsieh K-C, Chou F-F, Lee C-H. Nonsurgical treatment of thyroid injury after blunt cervical trauma.Am J Emerg Med. 2000;18:739–41. [PubMed]
4. Fontan FJ, Hernandez MS, Vazquez SP, et al. Thyroid gland rupture after blunt neck trauma. J Ultrasound Med. 2001;20:1249–51. [PubMed]
5. Rupprecht H, Rumenapf G, Braig H, et al. Acute bleeding caused by rupture of the thyroid gland following blunt neck trauma: case report. J Trauma. 1994;36:408–9. [PubMed]
6. Watson AP. Traumatic rupture of the thyroid gland. Aust Radiol. 1999;43:363–4.
7. Delikoukos S, Mantzos F. Thyroid storm induced by blunt thyroid gland trauma. Am Surg.2007;73:1247–9. [PubMed]
8. Behrends RL, Low RB. Acute goitre hematoma following blunt neck trauma. Ann Emerg Med.1986;16:1300–1. [PubMed]
9. Grace RH, Shilling JS. Acute haemorrhage into the thyroid gland following trauma and causing respiratory distress. Br J Surg. 1969;56:635–7. [PubMed]
10. Blaivas M, Hom DB, Younger JG. Thyroid gland haematoma after blunt cervical trauma. Am J Emerg Med. 1999;17:348–50. [PubMed]
11. Oertli D, Harder F. Complete traumatic transection of the thyroid gland. Surgery. 1994;115:527–9. [PubMed]
12. Oka Y, Nishijima J, Azuma T, et al. Blunt thyroid trauma with acute hemorrhage and respiratory distress. Emerg Med. 2007;32:381–5.
13. Hirshoren N, Hocwald E, Eliashar R. Isolated traumatic thyroid hemorrhage secondary to air bag deployment. Otolaryngol Head Neck Surg. 2004;130:791–3. [PubMed]
14. Hamid CH, Holland AJ, Cummins G, et al. Thyroid transection with spinal injury following blunt trauma in a child. Injury. 2004;35:332–5. [PubMed]
15. Skowsky WR. Toxic hematoma: an unusual and previously undescribed type of thyrotoxicosis.Thyroid. 1995;5:129–32. [PubMed]