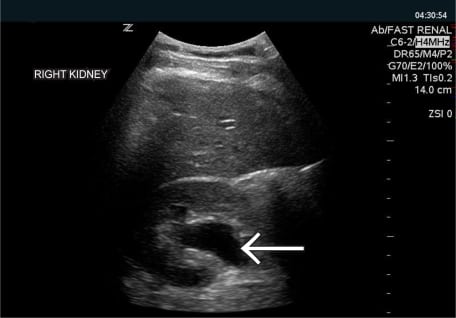
The focused assessment with sonography for trauma (FAST) exam is a routine diagnostic adjunct in the initial assessment of blunt trauma victims but lacks the ability to reliably predict which patients require laparotomy. Physiologic data play a major role in decision making regarding the need for emergent laparotomy versus further diagnostic testing or observation. The need for laparotomy often influences the decision to transfer the patient to a trauma center. We set out to derive a simple scoring system using both ultrasound findings and immediately available physiologic data that would predict which patients require laparotomy.
Brief alcohol intervention may improve outcomes for injury patients with hazardous drinking but is less effective with increased severity of alcohol involvement. This study evaluated a brief method for detecting problem drinking in minor trauma patients and differentiating hazardous drinkers from those with more severe alcohol problems.
Financial conflicts of interest have come under increasing scrutiny in medicine, but their impact has not been quantified. Our objective was to use the results of a national survey of academic emergency medicine (EM) faculty to determine if an association between money and personal opinion exists.
Although other specialties have examined the role of the chief resident (CR), the role and training of the emergency medicine (EM) CR has largely been undefined.
The healthcare chart is becoming ever more complex, serving clinicians, patients, third party payers, regulators, and even medicolegal parties. The purpose of this study was to identify our emergency medicine (EM) resident and attending physicians’ current knowledge and attitudes about billing and documentation practices. We hypothesized that resident and attending physicians would identify billing and documentation as an area in which residents need further education.
Injury is the leading cause of death and disability among the U.S. population aged 1 to 44 years. In 2006 more than 179,000 fatalities were attributed to injury. Despite increasing awareness of the global epidemic of injury and violence, a considerable gap remains between advances in injury-prevention research and prevention knowledge that is taught to medical students. This article discusses the growing need for U.S medical schools to train future physicians in the fundamentals of injury prevention and control. Teaching medical students to implement injury prevention in their future practice should help reduce injury morbidity and mortality. Deliberate efforts should be made to integrate injury-prevention education into existing curriculum. Key resources are available to do this. Emergency physicians can be essential advocates in establishing injury prevention training because of their clinical expertise in treating injury. Increasing the number of physicians with injury- and violence- prevention knowledge and skills is ultimately an important strategy to reduce the national and global burden of injury.
The objective of this study was to evaluate those factors, both intrinsic and extrinsic to the emergency department (ED) that influence two specific components of throughput: “door-to-doctor” time and dwell time.
Luxatio erecta humeri is an uncommon form of glenohumeral dislocation, resulting in the inferior displacement of the humeral head. Treatment with traction-counter traction techniques is usually successful in reducing most cases. We describe an unusual complication of this condition where initial reduction attempts of a luxatio erecta humeri repositioned the shoulder to an anterior dislocation position. After a thorough search of the literature, we were unable to find a similar case report of this type of complication during the reduction of a luxatio erecta shoulder dislocation.
The purpose of this study is to characterize the added value of the primary ICD-9 diagnosis assigned at the time of ED disposition compared to the chief complaint for patients with influenza-like illness (ILI).
A 38-year-old male presented to the Emergency Department (ED) after a motorcycle crash. The patient was unable to walk because of isolated left knee pain.
A 51-year-old male with hepatitis C and a history of intravenous (IV) drug use presented to the emergency department, reporting one day of worsening scrotal pain and swelling. He denied diabetes, trauma, or infection with HIV.
A 37-year-old woman presented to the emergency department with 12 hours of gradually worsening left lower quadrant pain with anorexia, vomiting, and diarrhea.
A previously healthy 25-year-old man presented to a community emergency department (ED) with two hours of sharp, intermittent, right-sided flank pain associated with hematuria. Vital signs showed no fever or tachycardia. Abdominal and genitourinary exam were benign.
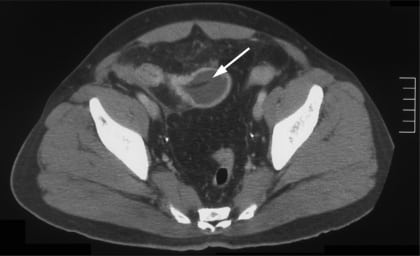
Necrotizing fasciitis (NF) is a rare and lethal soft tissue infection that requires urgent surgical intervention. It is most often found in the extremities occurring with precipitating trauma or in immunocompromised states. Signs and symptoms are often vague or missing making early diagnosis very difficult. Our patient presented with flank pain and altered mental status but no known precipitating factors. Computed Tomography showed gas within and around the right paraspinous muscle suspicious for NF. Given NF’s high lethality, early suspicion by emergency physicians of NF in patients with soft tissue infections or with systemic findings of unknown etiology is necessary.
To identify factors associated with culture-proven serious bacterial infection (SBI) and positive emergency department septic screening (EDSS) tests in children with bronchiolitis and to identify factors associated with the performance of EDSS.
To determine the incidence and frequency of follow-up instructions for incidental findings on computed tomography (CT) scanning of the abdomen and pelvis in trauma patients.
A 73-year-old man was brought to the emergency department (ED) after his caregiver noticed his percutaneous endoscopic gastrostomy (PEG) tube was missing.
A 31-year-old male presented to the emergency department with a chief complaint of headache after being assaulted with a baseball bat to the head. He denied loss of consciousness, nausea or vomiting.
A 31-year-old Caucasian female presented to the emergency department (ED) with chief complaint of a gradually progressive right extremity rash for past two days.
{kind=link}