
{kind=link}
| Author | Affiliation |
|---|---|
| Akira Hokama, MD, PhD | First Department of Internal Medicine, University of the Ryukyus, Okinawa, Japan |
| Kazuto Kishimoto | First Department of Internal Medicine, University of the Ryukyus, Okinawa, Japan |
| Yasushi Ihama | First Department of Internal Medicine, University of the Ryukyus, Okinawa, Japan |
| Hiroshi Chinen | First Department of Internal Medicine, University of the Ryukyus, Okinawa, Japan |
| Fukunori Kinjo | First Department of Internal Medicine, University of the Ryukyus, Okinawa, Japan |
| Jiro Fujita | First Department of Internal Medicine, University of the Ryukyus, Okinawa, Japan |
A 47-year-old man with a four-year history of ileo-colonic Crohn’s disease (CD) presented with abdominal pain and vomiting. On examination, his temperature was 38.2°C and a distended and generalized tender abdomen without peritoneal signs was noted. Laboratory tests revealed an increased white blood cell count of 10,000/mm3 and a C-reactive protein of 6.2 mg/dl. A plain abdominal radiograph revealed air-fluid levels in the small intestine. A computed tomography (CT) scan disclosed a circumlinear obstruction (arrow) in an ileal stricture with wall thickening (Figure 1). When questioned, the patient stated that his previous dinner consisted of dried cuttlefish and vegetable roots, which might be difficult to digest. Gastrointestinal decompression with nasoenteric tube and antibiotic treatment resolved his symptoms. The patient remained well and was discharged with maintenance infliximab treatment.
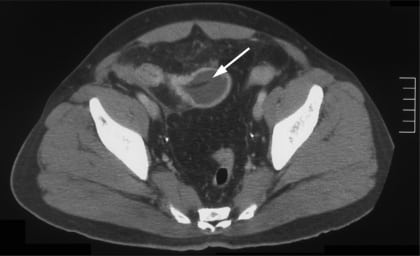
This case is an important reminder that CD patients are potentially at a greater risk of bowel obstruction with less digestible food. In other rare instances, bowel obstruction by food, fruit pits, phytobezoar or foreign bodies has actually led physicians to the diagnosis of CD.1–3 In these cases, a CT scan has been the key in assessing the bowel obstruction, providing a clear identification of the anatomical site to help identify the cause.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted August 11, 2009; Revision Received August 28, 2009; Accepted September 14, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Akira Hokama, MD, PhD. First Department of Internal Medicine, University of the Ryukyus, 207 Uehara, Nishihara, Okinawa 903-0215, Japan
Email: hokama-a@med.u-ryukyu.ac.jp
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Kaufman D, Lazinger M, Fogel S, et al. Fruit pit obstruction leading to the diagnosis of Crohn’s disease. Am J Surg. 2001;182:530. [PubMed]
2. Shedda S, Frizelle F. Images in clinical medicine. Crohn’s disease and an olive. N Engl J Med.2006;355:e22. [PubMed]
3. Slim R, Chemaly M, Yaghi C, et al. Silent disease revealed by a fruit–ileal obstruction. Gut.2006;55:181–90. [PMC free article] [PubMed]