
{kind=link}
| Author | Affiliation |
|---|---|
| Darlene Y. Robinson, MD | University of Maryland School of Medicine, Department of Emergency Medicine, Baltimore, MD |
| Amber V. Hamilton, BS | Loyola Marymount University, Los Angeles, CA |
A 73-year-old man was brought to the emergency department (ED) after his caregiver noticed his percutaneous endoscopic gastrostomy (PEG) tube was missing. It had been placed because of poor oral intake related to dementia. The caregiver stated that she last flushed the tube the day before and that the patient had been eating and drinking without difficulty. The patient was alert but disoriented. He appeared to be in no distress and could follow commands. His abdomen was soft, non-tender, and not distended, with good bowel sounds. The stoma site was intact, with no signs of infection. He was given an oral challenge and tolerated it well. As he was being prepared for discharge, the caregiver stated, “I still don’t know what happened to that tube. We looked for it everywhere!” Based on that new information, the treating physician requested an abdominal radiograph. It revealed that the PEG tube had migrated to the right lower abdomen (Figure). Computed tomography scan confirmed its location in the distal ileum and cecum. The patient was admitted to the hospital and managed conservatively. Serial radiographs tracked the tube’s migration, and it was expelled during defecation on the second day.

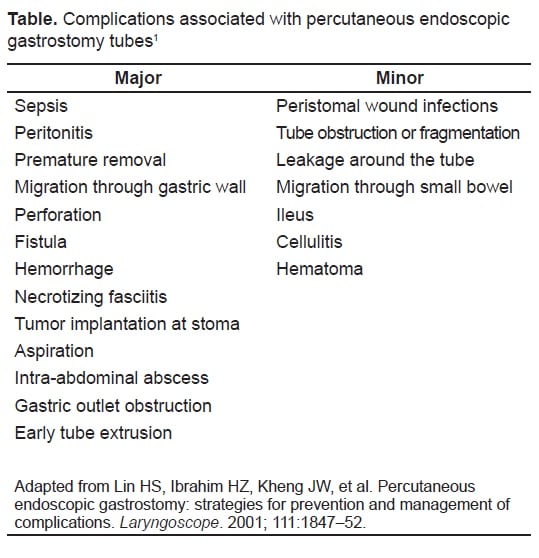
Debilitated and elderly patients may require placement of PEG tubes for nutritional support. Because many of them cannot communicate effectively, caregivers’ history becomes key to the diagnosis of complications. Complications associated with PEG tubes can occur upon insertion, during the immediate postoperative period, or after the tube has been in place for weeks, months, or years. We list the major and minor complications stemming from the disconnection and migration of PEG tubes in Table 1.1 The overall complication rate associated with PEG tubes has been reported as 4% to 24%.2 Major complications (those that require surgical intervention or are life threatening) emerge in 3% to 4% of tube recipients. Minor complications are more common, occurring in 7% to 20% of patients. Use of an external bumper decreases the likelihood of dislodgement and migration.3
In the ED, if a patient’s PEG tube cannot be found, the possibility of tube migration should be considered. Abdominal radiographs can confirm or exclude this condition. A patient with a PEG tube that has migrated into the intestinal tract can be managed conservatively but should be monitored for signs of obstruction and perforation. A foreign body such as a PEG tube can usually traverse the intestines if it passes the pylorus; however, passage through the ileocecal valve can lead to obstruction, necessitating surgical intervention.4
Footnotes
The manuscript was copyedited by Linda J. Kesselring, MS, ELS, the technical editor/writer in the Department of Emergency Medicine, University of Maryland School of Medicine, Baltimore, Maryland.
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted November 6, 2009; Revision Received November 13, 2009; Accepted November 16, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Darlene Y. Robinson, MD, Department of Emergency Medicine, University of Maryland School of Medicine, 110 South Paca Street, 6th Floor, Suite 200, Baltimore MD 21201
Email: darrobmd@aol.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Lin HS, Ibrahim HZ, Kheng JW, et al. Percutaneous endoscopic gastrostomy: strategies for prevention and management of complications. Laryngoscope. 2001;111:1847–52. [PubMed]
2. Lynch CR, Fang JC. Prevention and management of complications of percutaneuos endoscopic gastrostomy (PEG) tubes. Pract Gastroenterol. 2004;XXVIII:66, 68–70, 72–6.
3. Overstreet M. How does a PEG tube stay in? Nursing. 2004;34:21. [PubMed]
4. Hussien M, Fawzy M, Carey D. Percutaneous endoscopic gastroscopy tube migration: a rare cause of a common surgical problem. Int J Clin Pract. 2001;55:557–9. [PubMed]