
{kind=link}
| Author | Affiliation |
|---|---|
| Amandeep Singh, MD | Alameda County Medical Center – Highland Hospital, Department of Emergency Medicine, Oakland, CA |
| Jesus Alvarez, MD, MPH | Alameda County Medical Center – Highland Hospital, Department of Emergency Medicine, Oakland, CA |
A 77 year-old male presented to the Emergency Department with a complaint of progressive confusion over the past 4 days. His daughter accompanied him and noted that her father had difficulty remembering names, items, and dates and that he seemed to get frustrated when he was unable to recall these things. The patient reported that his symptoms began after he tried to relieve a feeling of ear congestion by forcibly exhaling while pinching his nose and closing his mouth. At that time he felt a loud pop and had improvement in his ear congestion. On exam the patient was noted to be alert and oriented, but had difficulty with word recall and had diminished sensation to his feet. A diagnostic computed tomography (CT) scan of his head was obtained which showed a spontaneous otogenic intracerebral pneumocephalus (Figure 1).
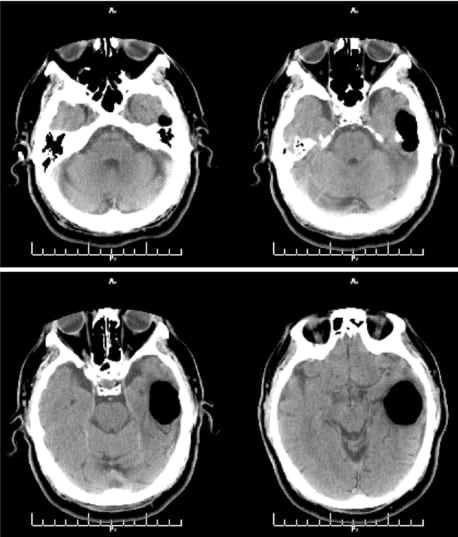
CT demonstrated a large collection of air in the anterior portion of the left middle cranial fossa that measures roughly 4 cm in greatest dimension. This collection is seen adjacent to the temporal bone and was thought to be secondary to rupture of the tegmen tympani or inguinal portion of the mastoid process of the temporal bone. The patient was transferred to a local tertiary care referral center where he underwent craniotomy with surgical decompression and obliteration of the dura air fistula.
Spontaneous otogenic intracerebral pneumocephalus is a rare event that has only been described about a dozen times in the medical literature.1,2 Raised pressure in the middle ear by nose blowing, sneezing, swallowing, coughing, or valsalva maneuver can create a positive pressure gradient, forcing air into the intracranial space, in susceptible individuals (i.e. those with congenital defects of the tegmen tympani or with chronic hyperpneumatization of the mastoid air cells). A “ball-valve effect” results and intracranial air can slowly build over a period of days to weeks. Left-sided lesions commonly present with intermittent confusion, forgetfulness, and expressive aphasia. In contrast, right-sided air pockets tend to present with headache, visual scotoma, hemiplegia or even syncope.1Treatment is generally surgical although conservative management has recently been described.3
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted October 28, 2009; Revision Received November 6, 2009; Accepted November 9, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Amandeep Singh, MD, Department of Emergency Medicine, 1411 East 31st Street, Oakland, CA 94602-1018
Email: asingh27@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Krayenbuhl N, Alkadhi H, Jung HH, et al. Spontaneous otogenic intracerebral pneumocephalus: case report and review of the literature. Eur Arch Otorhinolaryngol. 2005;262:135–8. [PubMed]
2. Villa RA, Capdevilla A. Spontaneous otogenic pneumocephalus. N Engl J Med. 2008;358:e13.[PubMed]
3. Schrijver HM, Berendse HW. Pneumocephalus by valsalva’s maneuver. Neurol. 2003;60:345–6.