
{kind=link}
| Author | Affiliation |
|---|---|
| Kenneth J. Perry, MD | SUNY Upstate Medical University, Department of Emergency Medicine, Syracuse, NY |
| Paul Ko, MD | SUNY Upstate Medical University, Department of Emergency Medicine, Syracuse, NY |
| Peter Mariani, MD | SUNY Upstate Medical University, Department of Emergency Medicine, Syracuse, NY |
| A. James Ciaccio, MD | Auburn Memorial Hospital, Department of Emergency Medicine, Auburn, NY |
A previously healthy 25-year-old man presented to a community emergency department (ED) with two hours of sharp, intermittent, right-sided flank pain associated with hematuria. Vital signs showed no fever or tachycardia. Abdominal and genitourinary exam were benign.
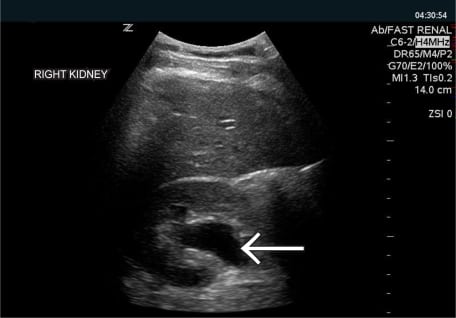
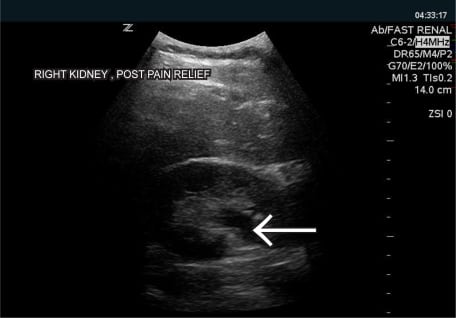
The patient was given analgesia while blood and urine samples were collected. Non-contrast computed tomography (CT) was ordered to evaluate suspected renal colic. The physician then performed bedside ultrasound (US) to evaluate for evidence of urinary obstruction. Multiple transverse views of the right kidney were obtained with the patient supine, using a Zonare z one system (Mountain View, CA) and a 4 MHz convex transducer. US findings were significant for moderate hydronephrosis (Figure 1). During US exam the patient felt instantaneous relief of his pain, which he described as a “pop.” Repeat US of the right kidney, 2.5 minutes following the first exam showed significant resolution of the previously imaged hydronephrosis (Figure 2).
CT results confirmed moderate right-sided hydronephrosis and a small obstructing calculus at the ureterovesical junction. Serum analysis showed normal renal function, and urine microscopy was significant for gross hematuria without pyuria. The patient remained pain free during a period of ED observation and was ultimately discharged.
Hydronephrosis can occur because of intraluminal, extramural, or functional urinary tract obstruction. These images are a first report of the rapid resolution time course of sonographic hydronephrosis in presumed ureteral stone passage. A literature review found that the time course of the resolution of hydronephrosis due to sudden relief of intraluminal obstruction in humans has not been demonstrated. The rapid resolution of hydronephrosis in this case is likely associated with the acute nature of the obstruction and the lack of any chronic underlying renal pathology in the patient.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted September 18, 2009; Accepted October 31, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Kenneth Perry, MD, Department of Emergency Medicine, SUNY Upstate Medical University, 550 E. Genesee St, Syracuse, NY, 13202
Email: perrykj@upstate.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.