Author Affiliation Corey Goldberg, MD University of Florida College of Medicine, Department of Emergency Medicine, Jacksonville, Florida Kathleen E. Carey, MD Mayo Clinic, Department of Radiology, Jacksonville, Florida Diagnosis A 34-year-old black man presented to the emergency department with right-sided pleuritic chest pain, productive cough, low grade fever, and dyspnea. He had a history of […]
Author Affiliation Kellee T. James, PharmD University of California San Francisco, Department of Clinical Pharmacy, San Francisco, California Alissa Detz, MD Robert Wood Johnson Foundation Clinical Scholar, University of California Los Angeles, Department of Medicine, Los Angeles, California Zlatan Coralic, PharmD University of California San Francisco, Department of Clinical Pharmacy, San Francisco, CaliforniaUniversity of California […]
Author Affiliation Alexander J. Scumpia, DO, MSc Mount Sinai Medical Center, Department of Emergency Medicine, Miami, Florida Daniel A. Aronovich, DO Mount Sinai Medical Center, Department of Emergency Medicine, Miami, Florida Loredana Roman, BS Victor Babes University of Medicine and Pharmacy, Department of Medicine, Timisoara, Romania Vanitha Vasudevan, MD Ryder Trauma Center, Department of Surgery, […]
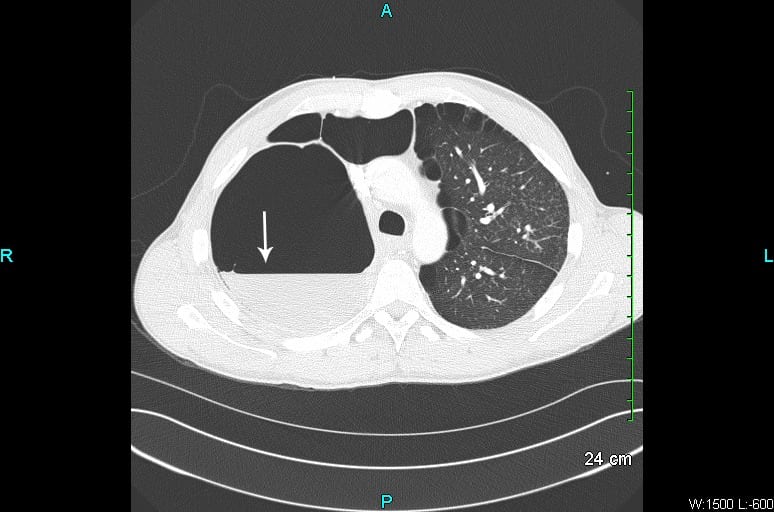
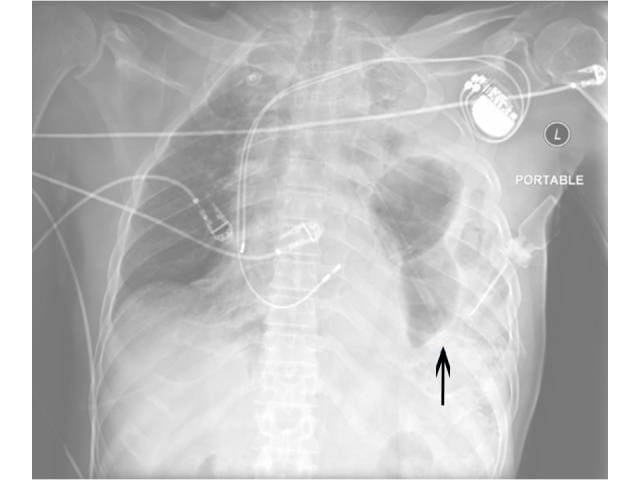
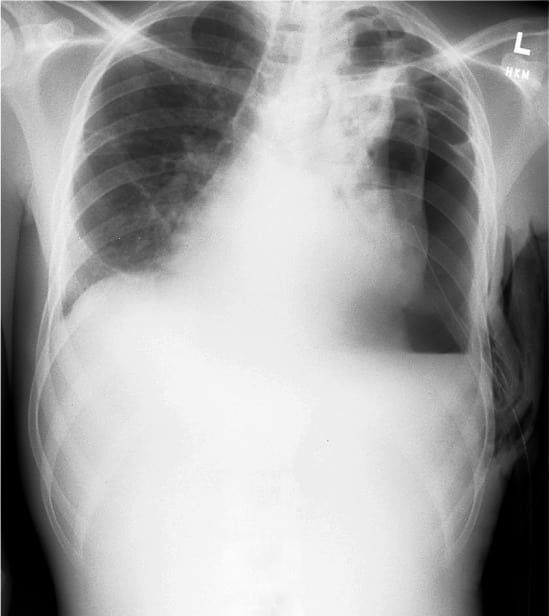
Tuberculosis (TB) is a known cause of secondary pneumothorax. In areas with endemic TB, complications from the disease, including pneumothorax, are increasing in prevalence. We present the cases of 3 patients (ages 32 years, 17 years, and 3 months) seen in the emergency department at John F. Kennedy Medical Center in Monrovia, Liberia, West Africa. Each presented with shortness of breath and cough, and with some degree of respiratory distress. Airway compromise was present with tracheal or mediastinal deviation. Each patient underwent tube thoracostomy with improvement in pneumothorax and respiratory status.
A 20-year-old-female presented to the emergency department (ED) with a chief complaint of a persistent dull headache associated with a 7 mm dilated, non-reactive right pupil, and occasional blurry vision for 4 days. The patient had a past medical history significant for Noonan’s syndrome (NS).
A 15-year-old female presented to the emergency department (ED) with a 1-week history of fevers, vomiting, back pain and dysuria. Her primary care physician started her on cefdinir for a urinary tract infection. On initial evaluation she was febrile, tachycardic, and had an exam notable for tenderness of both the left costovertebral angle and suprapubic region.
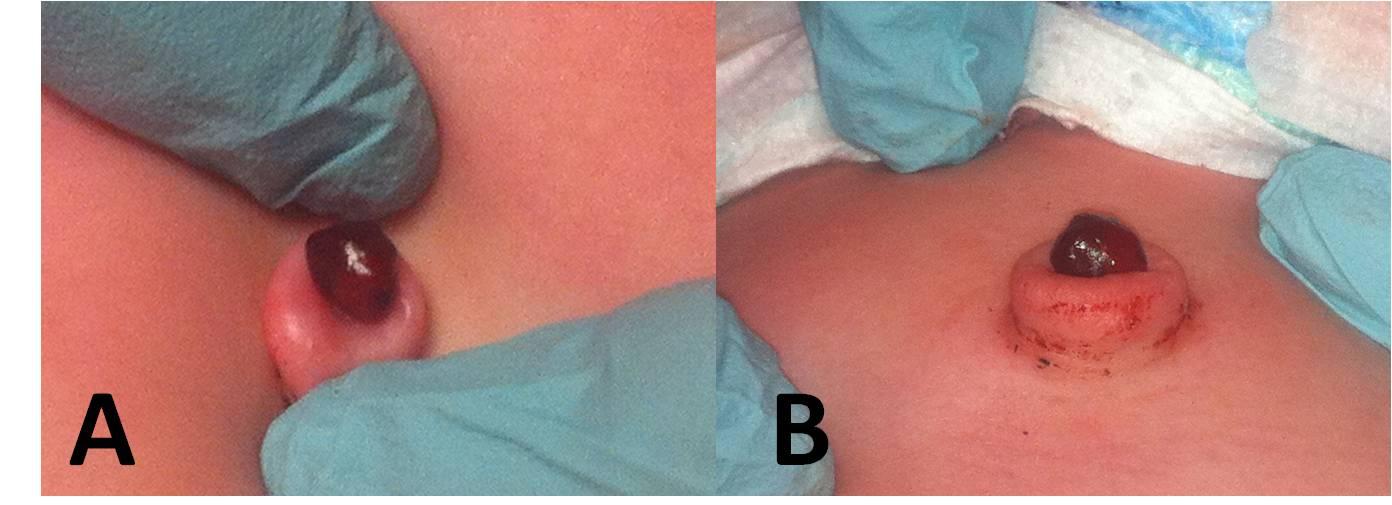
A 41-day-old girl presented to the emergency department with a new dark red mass protruding from the umbilicus noted 3.5 hours prior to presentation. The patient’s mother reported the umbilical stump fell off at 4 days of life, but the patient continued to have intermittent clear green drainage from a small mass at the base of the umbilicus. The patient was born full-term with an otherwise unremarkable medical history.
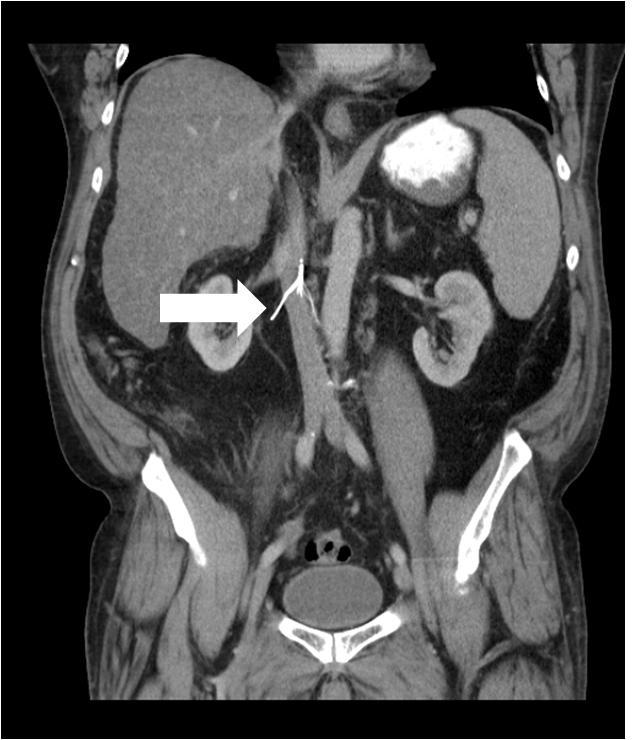
A 46-year-old male with diabetes, hypertension, and a history of pulmonary embolism (status post placement of a retrievable Celect inferior vena cava [IVC] filter) presented to the emergency department with progressively worsening abdominal pain for 1 month.
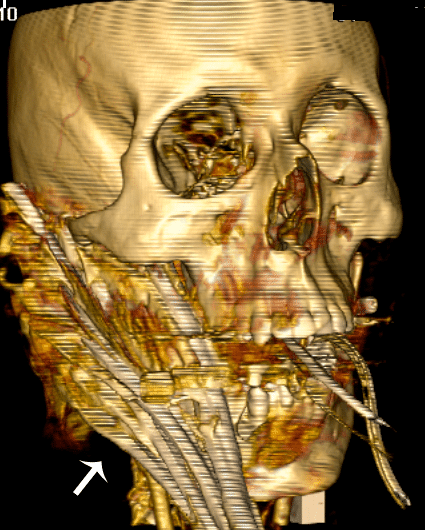
Penetrating injuries to the face or neck can cause difficult airway issues. There is a relative dearth of literature to define the best approach to these patients. Impalement injuries are uncommon, and survivable injuries are most commonly confined to the abdomen or thorax. We report the case of a patient with an obviously difficult airway due to a facial impalement (Jael’s Syndrome) injured at a local construction site.
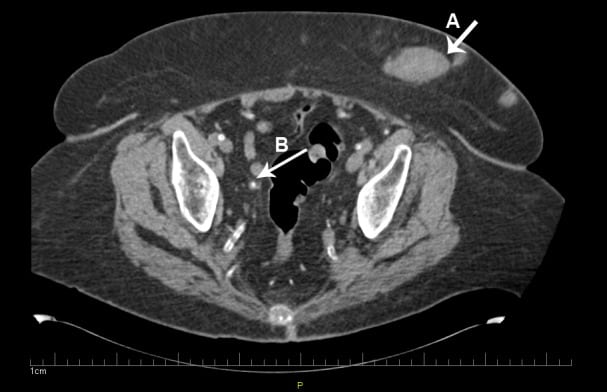
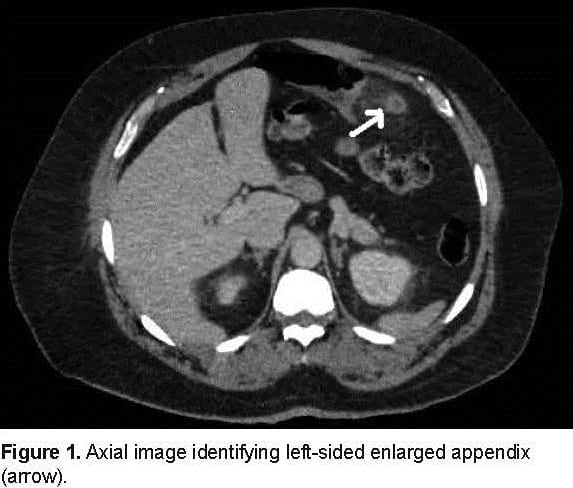
An 81-year-old female with history of end stage renal disease on hemodialysis presented with worsening of abdominal pain of 2 days’ duration. The pain started as a dull ache over the lower abdomen 2 months earlier, diffuse but especially prominent over the lower quadrant, and was unrelieved by analgesic medications.
A 49-year-old man was brought to the emergency department by ambulance after he sustained a stab wound to the chest. He was alert but diaphoretic, with an initial systolic blood pressure of 90 by palpation and a heart rate of 110. A 1 cm laceration was noted at the left lower sternal border. Lung sounds were clear bilaterally, and heart sounds were muted.
Idiopathic intracranial hypertension (IIH), also known as pseudotumor cerebri, defined as elevated intracranial pressure with no evident cause found on extensive evaluation.
A 40-year-old man with Hepatitis C and a history of cocaine abuse presented with multiple stages of painful rashes on his extremities and ears. On examination, the patient had several areas of purpuric macules and retiform purpura to his legs and ears, as well as large ulcerations with erythematous borders on bilateral lower extremities
A 76-year-old man with a history of ankylosing spondylitis presented to the emergency department complaining of neck pain. He stated the pain began when he slipped to the ground from a seated position in his bedroom.
A 36-year-old male presented to the emergency department (ED) complaining of “lumps in my penis.” The patient described 2 firm, raised areas on the dorsum of his penis that had been present 1 week. He had no pain at rest or with palpation but mild discomfort with erection. He denied trauma, dysuria, hematuria, or discharge. He had no prior medical history and took no medications.
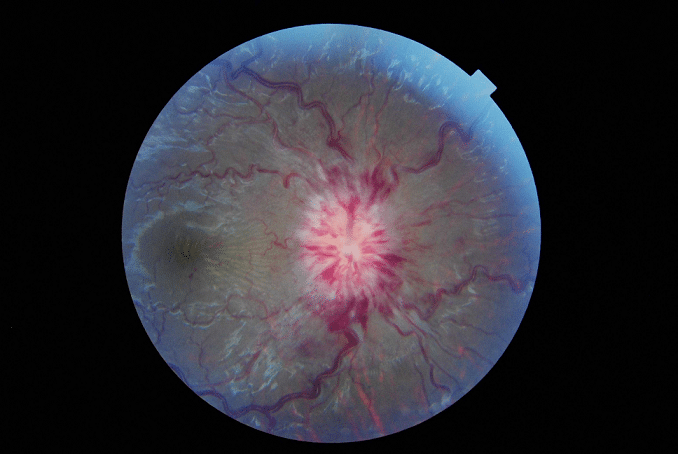
A 33-year-old woman with no past medical history presented to the emergency department with asymmetric pupils. At 7:30am while putting on makeup, she noted her pupils were equal in size. One hour later, she developed light sensitivity in her right eye, and soon after noticed her right pupil was significantly enlarged. She denied headache, facial or extremity weakness, dysarthria, or ataxia. On exam…
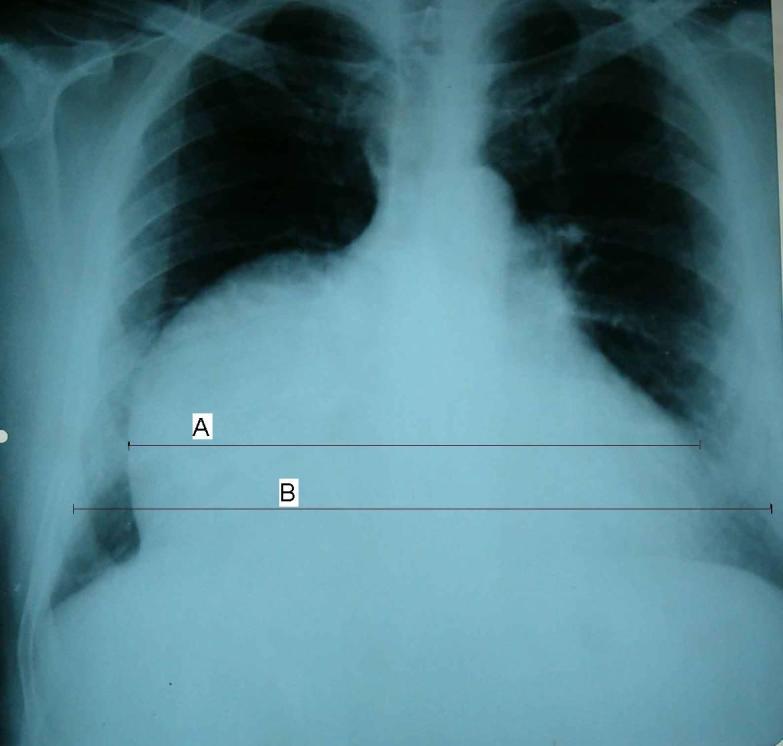
A 29-year-old man with sudden onset of dyspnea and chest pain with impairment of the general status after falling down from five meters was transferred to our emergency department. He was completely asymptomatic before the injury, but hypotensive (80/50 mmHg) and tachycardic (112 beats/minute) after the injury. Chest radiograph revealed a bulging cardiac silhouette on the right paracardiac region with an increased cardiothoracic ratio of 70%.
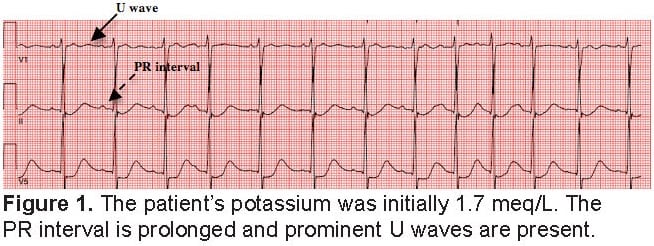
Thyrotoxic periodic paralysis (TPP) attacks are characterized as recurrent, transient episodes of muscle weakness that range from mild weakness to complete flaccid paralysis. In this case study, we followed a patient’s potassium levels analyzing how they correlate with electrocardiogram changes seen while treating his hypokalemia and ultimately his paralysis.
A 38-year-old Hispanic woman with no known past medical or family history presented to the emergency department with severe, intractable left upper and lower extremity pain and inability to walk for 2 days. The woman reported a history of chronic, progressive left hand, arm, and leg deformity over the previous 2 years with episodic flares of severe pain. Physical exam…
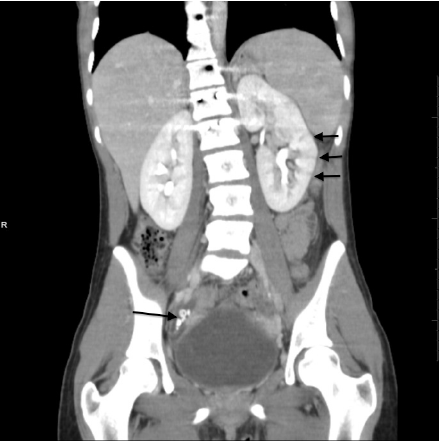
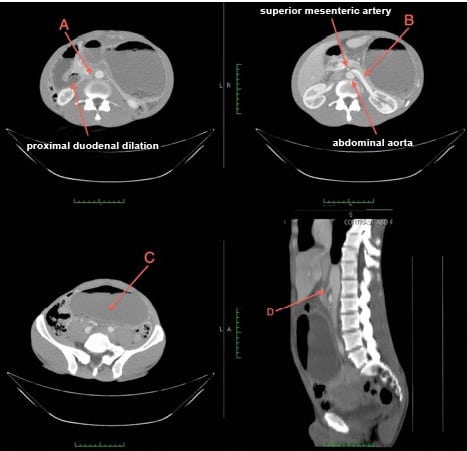
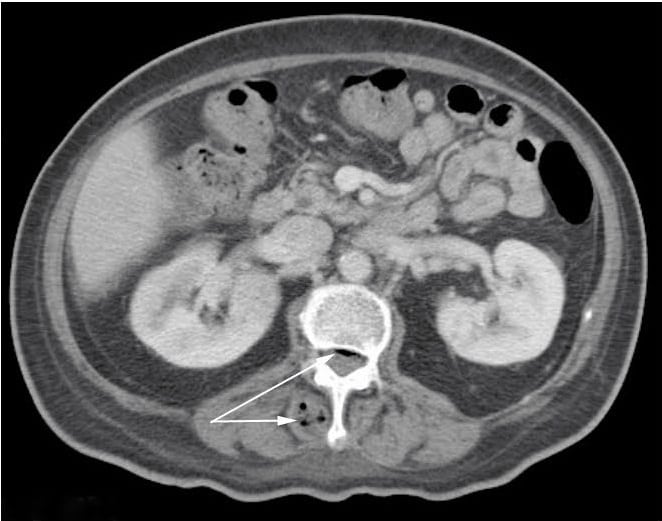
Superior mesenteric artery (SMA) syndrome is a rare cause of abdominal pain, nausea and vomiting that may be undiagnosed in patients presenting to the emergency department (ED). We report a 54-year-old male presenting to a community ED with abdominal pain and the subsequent radiographic findings.The patient’s computed tomgraphy (CT) of the abdomen and pelvis demonstrates many of the hallmark findings consistent with SMA syndrome, including; compression of the duodenum between the abdominal aorta and superior mesenteric artery resulting in intestinal obstruction, dilation of the left renal vein, and gastric distension.
A 67-year-old woman presented to the emergency department in congestive heart failure. She also had a history of transverse myelitis, which had caused her to be bedbound with an indwelling urinary catheter. During the physical examination, the urine in her Foley tubing and bag were noted to be bright purple. When asked…
A 63-year-old female with a past medical history of hepatitis C and cirrhosis presented to the emergency department with a four-month history of increased swelling and tenderness to the right clavicle. The patient was afebrile with a firm, warm area measuring 6 cm x 4.5 cm x 2 cm, located over the medial right clavicle. The patient had a remote history of…
A 50-year-old woman with a history of non-insulin dependent diabetes mellitus (NIDDM) presented to the emergency department (ED) with right hip pain for 1 week. The pain was described as constant, non-radiating, and worse with weight bearing. She denied any trauma, fevers, intravenous drug use, or recent surgery. Physical exam revealed…
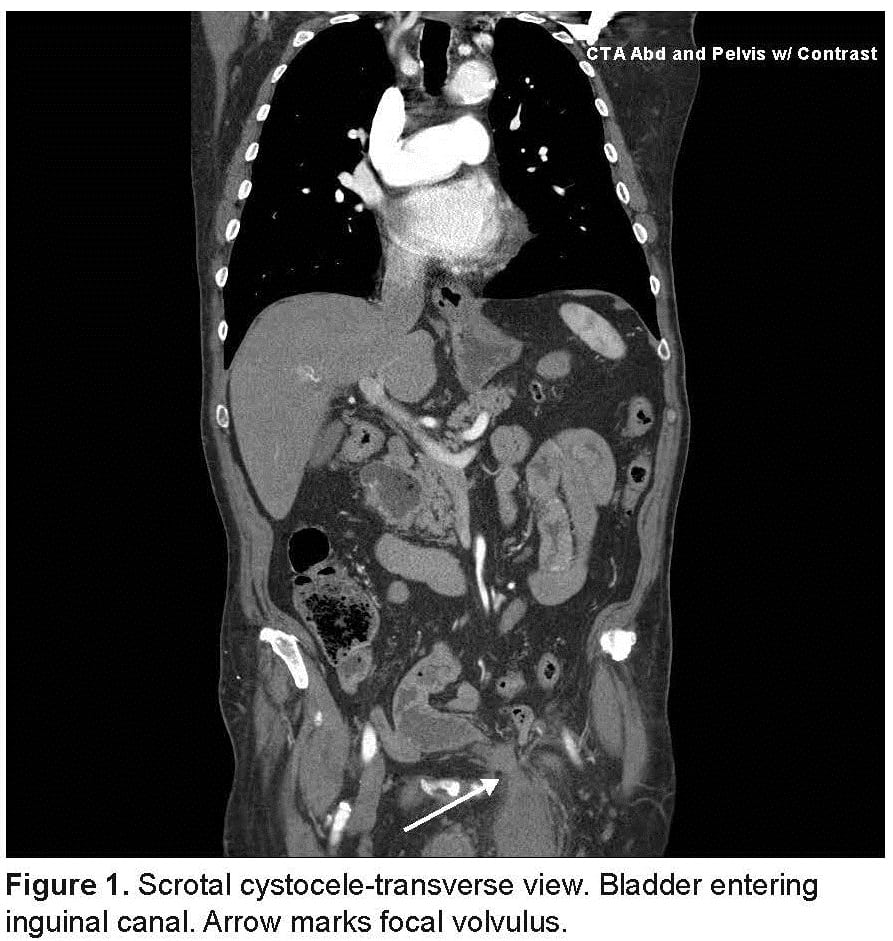
A 77-year-old male presented to our emergency department (ED) with a 3-hour history of acute severe lower abdominal pain, inability to void, a swollen scrotum, and one episode of vomiting. His relevant past medical history included: hypertension, diabetes mellitus, and distant right inguinal hernia repair. Vital signs were: 96.4° F, 101, 22, and 205/90. Examination revealed a…
{kind=link}