
{kind=link}
| Author | Affiliation |
|---|---|
| Nathan Borden, MD | Carl R. Darnall Army Medical Center, Department of Emergency Medicine, Fort Hood, Texas |
| Derek Linklater, MD | Carl R. Darnall Army Medical Center, Department of Emergency Medicine, Fort Hood, Texas |
A 15-year-old female presented to the emergency department (ED) with a 1-week history of fevers, vomiting, back pain and dysuria. Her primary care physician started her on cefdinir for a urinary tract infection. On initial evaluation she was febrile, tachycardic, and had an exam notable for tenderness of both the left costovertebral angle and suprapubic region. Her urinalysis had 25 white blood cells, leukocyte esterase 75 leu/μL, and protein 50 mg/dL. While in the ED, the patient continued to experience bouts of emesis despite fluid resuscitation and anti-emetics. Repeat examination showed developing right lower quadrant tenderness without guarding or rebound. An intravenous contrast computed tomography (CT) was performed (Figure).
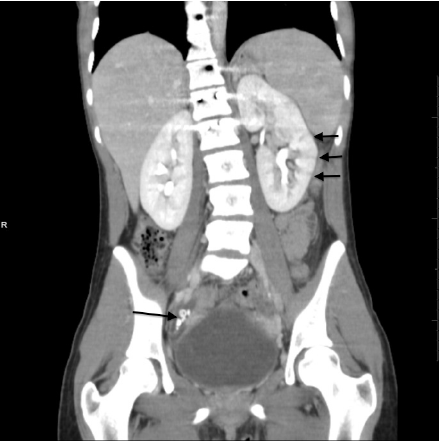
Intravenous-contrast enhanced computed tomography of the abdomen and pelvis. Three short arrows illustrate residual contrast in the parenchyma of the left kidney. This is a striated nephrogram and is consitent with acute pyelonephritis. The long arrow shows several appendicoliths in a dilated appendix. This is consistent with acute appendicitis.
The CT (Figure) shows residual contrast in the parenchyma of the left kidney (a “striated nephrogram”) consistent with pyelonephritis. The appendix contains multiple appendicoliths and is both dilated and inflamed; this is consistent with acute appendicitis. This case illustrates the dulling of Ockham’s razor and serves as a reminder that sometimes Hickam’s Dictum (“Patients can have as many diseases as they damn well please”) prevails over diagnostic parsimony. More importantly, physicians are reminded to pursue alternate or additional diagnoses when the patient’s symptoms cannot be explained by a single, unified diagnosis — in this case acute pyelonephritis.1 Thinking broadly in the face of contradictory data helps to prevent the most common cognitive error in medicine: satisfaction of search. Satisfaction of search refers to the tendency to stop looking once something is found.2 Attributing the right lower quadrant pain to cystitis conforms to Ockham’s razor, but leaves one vulnerable to satisfaction of search, and in this case would have missed an additional diagnosis.
Footnotes
Supervising Section Editor: Sean O. Henderson, MD
Submission history: Submitted September 4, 2012; Revision received September 17, 2012; Accepted October 22, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.10.12164
Address for Correspondence: Nathan Borden, MD, Carl R. Darnall Army Medical Center, Department of Emergency Medicine, 36000 Darnall Loop, Fort Hood, TX 76544. Email: nate.borden@gmail.com.
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none. The opinions expressed in this article are those of the authors and do not reflect the official policy of the Department of the Army, Department of Defense, or the U.S. Government.
REFERENCES
1. Groopman J. How Doctor’s Think. Houghton Mifflin; 2007.
2. Croskerry P. Achieving quality in clinical decision making: Cognitive strategiesand detection of bias. Acad Emerg Med. 2002;7(9):1184–1204. [PubMed]