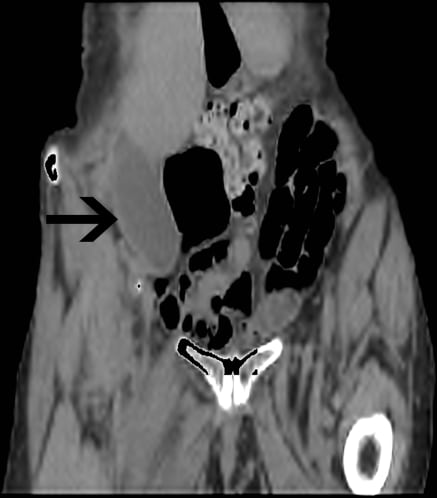
A 23-year-old male with a history of Crohn’s disease and prior ileostomy, presented to the emergency department complaining of his “intestines coming out.”
A 60-year-old man had just enjoyed a summer meal that included hamburgers, fruit, and lettuce salad. He finished it off with some ice cream, and to make it healthier he threw on it a handful of seeds from the cupboard that he understood to be flax seeds.
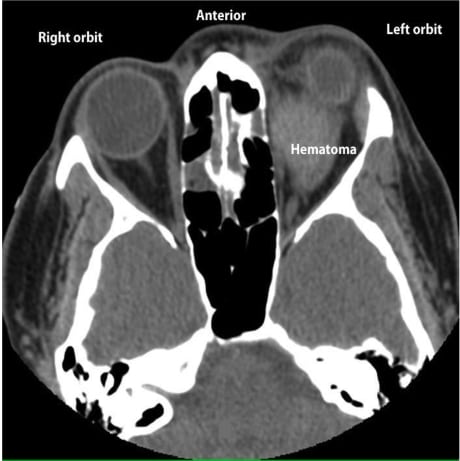
The following case describes a 26-year-old female who presented to the emergency department with a nontrauamtic retrobulbar hematoma associated with warfarin toxicity. The application and limitations of focused bedside ocular sonography for this condition are discussed.
Toxic epidermal necrolysis is a rare disease that is most often drug-induced but can be of idiopathic origin. We present a case that originated at the site of a cigarette burn to the forearm and review the key elements of physical exam findings and management of this life-threatening dermatological condition, which needs to be promptly recognized to decrease patient mortality.
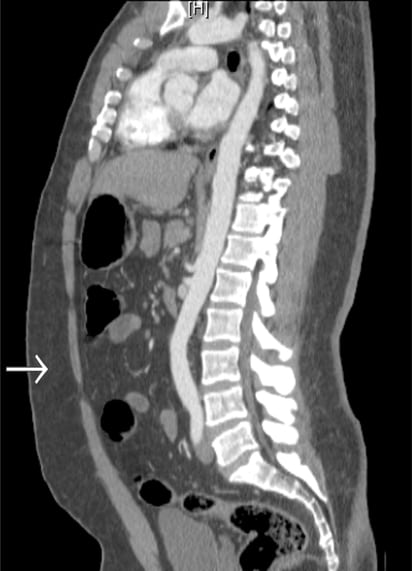
Repeat visits to an emergency department (ED) within a short period of time for recurring or continuing abdominal pain should make physicians suspicious for relapsing or episodic disease processes. I present a case of a 17-year-old female with cecal volvulus found only after multiple ED visits.
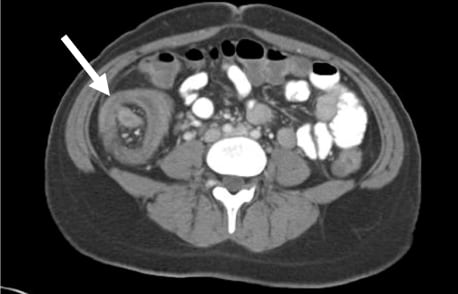
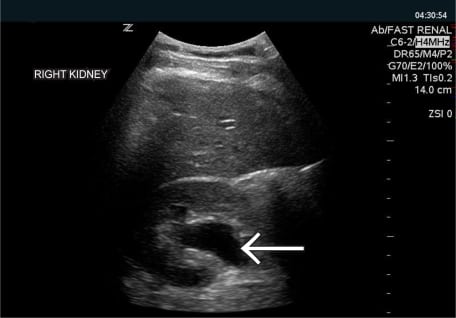
Intussusception is a condition found primarily in the pediatric population. In the adult population, however, intussusception is usually due to a pathological process, with a higher risk of bowel obstruction, vascular compromise, inflammatory changes, ischemia, and necrosis. Radiographic and sonographic evidence can aid in the diagnosis. Surgical intervention involving resection of affected bowel is the standard of care in adult cases of intussusception.
A 38-year-old male presented to the Emergency Department (ED) after a motorcycle crash. The patient was unable to walk because of isolated left knee pain.
A 51-year-old male with hepatitis C and a history of intravenous (IV) drug use presented to the emergency department, reporting one day of worsening scrotal pain and swelling. He denied diabetes, trauma, or infection with HIV.
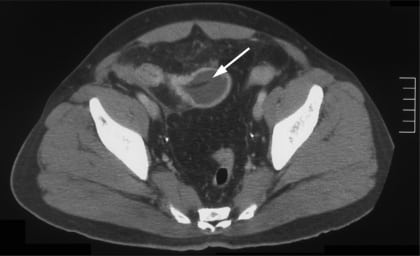
A 37-year-old woman presented to the emergency department with 12 hours of gradually worsening left lower quadrant pain with anorexia, vomiting, and diarrhea.
A previously healthy 25-year-old man presented to a community emergency department (ED) with two hours of sharp, intermittent, right-sided flank pain associated with hematuria. Vital signs showed no fever or tachycardia. Abdominal and genitourinary exam were benign.
A 73-year-old man was brought to the emergency department (ED) after his caregiver noticed his percutaneous endoscopic gastrostomy (PEG) tube was missing.
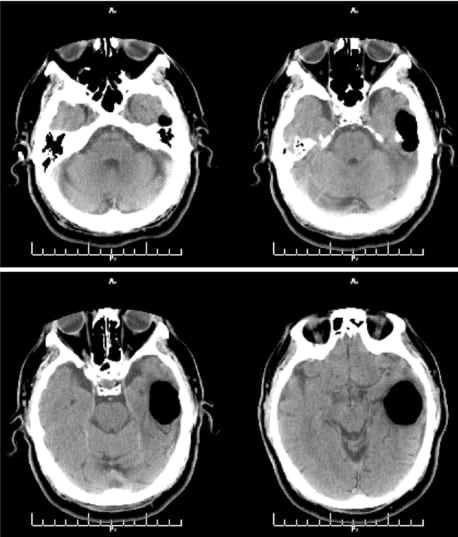
A 31-year-old male presented to the emergency department with a chief complaint of headache after being assaulted with a baseball bat to the head. He denied loss of consciousness, nausea or vomiting.
A 31-year-old Caucasian female presented to the emergency department (ED) with chief complaint of a gradually progressive right extremity rash for past two days.
A 68-year-old male presented to the emergency department with anterior right knee pain after falling at home and directly hitting his patella on the stepladder edge while he was going upstairs.
Guillain Barré Syndrome (GBS), although an uncommon diagnosis in the emergency department (ED), usually presents as one of the more common chief complaints—weakness. In this report we present an unusual case of weakness, initially seen in the ED and sent home only to return with worsening symptoms and ultimately found to be GBS.
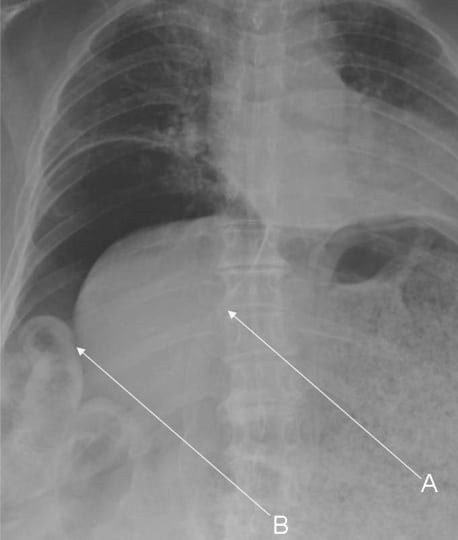
This case report describes a patient with a subacute right-sided tension hemopneumothorax following an occult stab. The patient’s electrocardiogram (ECG), performed as part of a standardized triage process, demonstrated significant abnormalities that misguided initial resuscitation, but resolved following evacuation of the tension hemopneumothorax. Tension pneumothorax is typically regarded as an immediately life-threatening condition that requires emergent management with needle or tube thoracostomy. However, we believe that subacute tension pneumothorax may be a rarely observed clinical phenomenon and may lead to unique ECG findings. We believe that the ECG changes we observed provided an early clue to the eventual diagnosis of a subacute tension pneumothorax and have not been previously described in this setting.
{kind=link}