
{kind=link}
| Author | Affiliation |
|---|---|
| Katherine W. Davisson, MS4 | University of Vermont College of Medicine, Burlington, VT |
| George L. Higgins, III, MD | Department of Emergency Medicine, Maine Medical Center, Portland, ME |
| Michael W. Jung, MD | Department of Emergency Medicine, Maine Medical Center, Portland, ME |
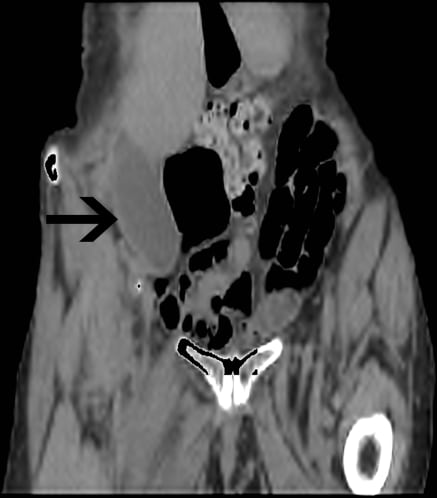
An 81-year-old Caucasian woman presented to the emergency department (ED) complaining of right groin pain of one month’s duration. She was able to bear weight but was finding it increasingly difficult to ambulate. She described a vague history of falling, prompting a prior negative work-up for hip fracture. In the ED, she was noted to be kyphotic, but exhibited no signs of trauma. Exam revealed tenderness to deep palpation in the right lower quadrant without rebound or mass. She had full range of motion of her right hip with minimal discomfort, but hip extension elicited a positive psoas sign. Given concern about the possibility of either an occult hip fracture or a subacute presentation of appendicitis, imaging studies were ordered.
The patient had an inflamed pelvic gallbladder. Anatomic malposition of organs can result in unusual clinical presentations. Abnormalities in the gallbladder mesentery, including a wide mesentery, absent mesentery or mesentery covering only the cystic duct and artery, can result in a “floating” or “hanging” gallbladder, predisposing it to torsion. Factors associated with this condition include atrophy of the liver, loss of visceral fat and elasticity with aging, weight loss, and kyphosis. Triggering events for torsion include violent peristalsis of neighboring organs, as well as atherosclerosis and tortuosity of the cystic artery.1–3 Torsion is most common in the elderly with a female-to-male ratio of 3:1 and can be incomplete, causing intermittent pain, or complete, with resultant gangrene or rupture.2 Laboratory data are typically not helpful. Ultrasound and computed tomography imaging often demonstrate an enlarged, thickened-walled gallbladder located outside its normal anatomic fossa.3 Most patients with torsion have no gallstones. Torsion or inflammation of a hanging pelvic gallbladder should be considered in the differential diagnosis of an elderly, kyphotic female patient with right lower quadrant or pelvic pain.
Footnotes
Supervising Section Editor: Rick McPheeters, MD
Submission history: Submitted December 4, 2009; Revision January 4, 2010; Accepted January 11, 2010
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: George L. Higgins III, MD, Department of Emergency Medicine, Maine Medical Center, 47 Bramhall Street, Portland, Maine 04102
Email: higgig@mmc.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Cho YP, Kim HJ, Jung SM, et al. Torsion of the Gallbladder: Report of a Case. Yonsei Med J.2005;46(6):862–5. [PMC free article] [PubMed]
2. Hahn RG, Connor PD. Pelvic Pain from Cholelithiasis in a Patient with Kyphoscoliosis. Am Fam Physician. 1995;51(4):750, 752. [PubMed]
3. Tarhan OR, Barut I, Dinelek H. Gallbladder Volvulus: Review of the literature and report of a case.Turk J Gastroenterol. 2006;17(3):209–11. [PubMed]