
{kind=link}
| Author | Affiliation |
|---|---|
| Clark Rosenberry, MD | Madigan Army Medical Center, Department of Emergency Medicine, Fort Lewis, WA |
| Vincent Ball, MD | Madigan Army Medical Center, Department of Emergency Medicine, Fort Lewis, WA |
A 43-year-old man presented to the emergency department (ED) with epigastric pain radiating down the center of his abdomen. He denied significant use of alcohol or non-steroidal anti-inflammatory drugs. He had uncontrolled hypertension on hydrochlorothiazide and a blood pressure of 185/95 mmHg. A two-dimensional aortic ultrasound was done at the patient’s bedside and revealed a double lumen and an intimal flap on the longitudinal axis (Figure 1). The transverse view was limited due to body habitus and bowel gas.
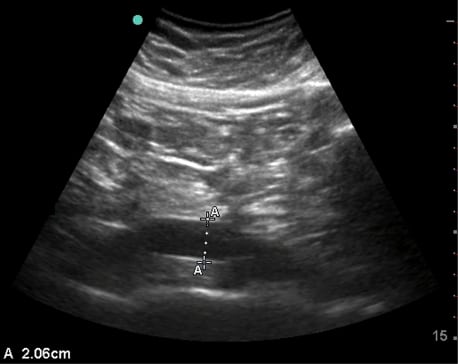
Subsequent aortic computed tomography (CT) revealed an inflamed pancreatic head and a normal aorta (Figure 2). Lipase was elevated (1063 units/L). This patient’s aorta appeared as a false positive abdominal aortic dissection on bedside ED ultrasound. Radiologists refer to this aorta as normal despite its curvature. There is a case report of a tortuous thoracic aorta that led to a false positive descending thoracic aortic dissection on transesophageal echocardiogram.1 Severe tortuosity is usually seen in the thorax and may be associated with aortic aneurysms; however, this patient’s curvature does not indicate pathology. The abnormal curvature in this patient’s distal aorta allows for the impression on ultrasound that there is a false lumen and aneurysmal dilation. The retroaortic tissue appears to be a false lumen.
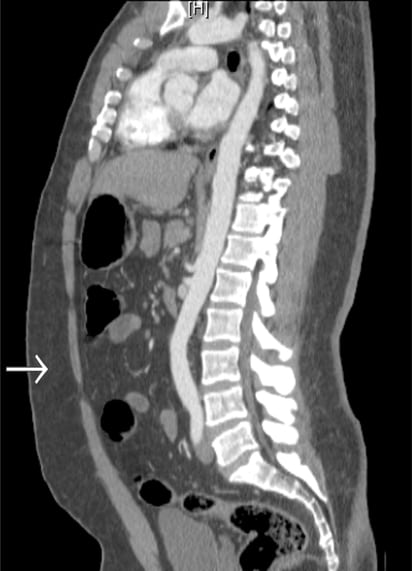
There is also the appearance of an intimal flap and communication with the false lumen on ultrasound. These findings are likely due to artifact created by overlying bowel gas, which is present directly above that segment of the aorta as seen on CT scan. Other explanations for the flap are less likely. First, the bifurcation of the aorta into the iliac arteries is farther caudal. Second, the inferior vena cava lies well to the right of this aorta and would not be seen as dorsal with our midline abdominal probe orientation. Third, there is only minimal curvature of the aorta in the coronal plane. Lastly, the only tissues directly surrounding this segment of the aorta are lymph nodes.
False positive abdominal aortic dissections due to artifact associated with color Doppler ultrasound have been described,2,3 and false positives can occur with two-dimensional ultrasound.4,5 Our case is novel in that no reported instances of false positive abdominal aortic dissection on two-dimensional ultrasound are associated with an abnormal curvature of the aorta. This case emphasizes the importance of having multiple views on ultrasound to properly delineate anatomy. The transverse images of this patient’s aorta did not clearly reveal the vessel lumen, making our scan a limited one. The patient was ultimately admitted for pancreatitis, and the curvature in his aorta was an incidental finding.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted September 9, 2009; Revision Received October 2, 2009; Accepted November 16, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Clark Rosenberry, MD, 245 St. Helens Ave, Apt 609, Tacoma, WA 98402
Email crosenberry04@jcu.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Katz E, Applebaum R, Earls J, et al. Tortuosity of the descending thoracic aorta simulating dissection on transesophageal echocardiography. J Am Soc Echocardiogr. 1997;10:83–7. [PubMed]
2. Crotty JM, Timken MJ. Pseudodissection of the abdominal aorta on color Doppler imaging. J Ultrasound Med. 1995;14:853–7. [PubMed]
3. Nguyen BD, Hamper UM. False positive dissection of abdominal aortic aneurysm by color Doppler duplex ultrasonography. J Ultrasound Med. 1995;14:467–9. [PubMed]
4. Victor MF, Mintz GS, Kotler MN, et al. Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol. 1981;48:1155–9. [PubMed]
5. Roudaut R, Billes MA, Gosse P, et al. Echocardiographic diagnosis of aortic dissection. Limits, pitfalls and difficulties. Arch Mal Coeur Vaiss. 1987;80:1793–9. [PubMed]