
{kind=link}
| Author | Affiliation |
|---|---|
| Joel A. Miller, MD | Carl R. Darnall Army Medical Center, Department of Emergency Medicine, Ft. Hood, TX |
| Marc E. Levsky, MD | Seton Medical Center, Division of Emergency Medicine, Daly City, CA |
| Melissa L. Givens, MD, MPH | Carl R. Darnall Army Medical Center, Department of Emergency Medicine, Ft. Hood, TX |
| Michael A. Miller, MD | Tripler Army Medical Center, Department of Emergency Medicine, Honolulu, HI |
ABSTRACT
Introduction:
Laryngeal mask airways (LMAs) are often used as airway rescue devices where laryngoscopy is difficult. The LMA does not protect the airway and is preferably replaced with a cuffed endotracheal tube. There are reports of cases where an Eschmann tracheal tube introducer (ETTI) was successfully used to bridge between a standard LMA and an endotracheal tube. This project was designed to determine whether an Eschmann stylet can reliably be passed through an LMA into the trachea as a means of rescue intubation.
Methods:
Nineteen emergency medicine residents and attending physicians, who were participants in a cadaveric airway course, placed and inflated a size 4 LMA (The Laryngeal Mask Company Ltd., San Diego, CA) on each of six unembalmed human cadavers in the usual fashion. They then attempted to pass a lubricated, 15 Fr, reusable, coude-tipped ETTI (Portex, Smiths Medical, Keene, NH)) through the airspace/handle of the inflated LMA. The LMA was then deflated and removed while the ETTI was held in place. Investigators then determined the location of the ETTI by laryngoscopy.
Results:
Of 114 attempts at the rescue procedure, 59 resulted in placement of the bougie into the trachea, yielding an overall success rate of 52% (95% CI 48%–56%). There were no significant differences in performance based on level of training of residents or years of experience of attending physicians.
Conclusion:
While not a primary difficult airway option, the use of a ETTI as a bridge device between LMA and endotracheal tube was successful about 50% of the time.
INTRODUCTION
Larngeal masks airways (LMA) are frequently used in the emergency department (ED) as an airway rescue device, to help ventilate patients when endotracheal intubation is impossible. They are especially useful in cases where the laryngoscopic view is limited by inability to optimally position a patient’s neck, as in cases of trauma. Although the LMA may make ventilation easier, it does not protect the airway the way a cuffed endotracheal tube does, and thus it is desirable to transition to a cuffed endotracheal tube as soon as feasible. The intubating LMA (I-LMA), or LMA Fastrach™ (LMA North America, Inc., San Diego, CA) was invented for this purpose.
Anecdotal experience of the authors, as well as reports in the literature,1 have included using an Eschmann tracheal tube introducer (ETTI), sometimes called a gum elastic bougie,2 as a bridge device between a standard (classic, non-intubating) LMA and a cuffed endotracheal tube in an emergency airway setting. This maneuver is performed by inserting a lubricated ETTI down the ventilating lumen/handle of the LMA, hopefully directing it into the trachea. The LMA is then withdrawn, while holding the ETTI in place. The endotracheal tube is then railroaded down the ETTI into the trachea, and placement is confirmed in the usual fashion. This procedure could achieve the same result as the I-LMA device, in situations where only a classic LMA is available.
The goal of this investigation is to determine how often one might expect an ETTI placed down the lumen of an LMA to be positioned in the trachea and thus aid in completing a difficult airway. If LMA-guided ETTI placement is frequently successful, this technique might be of value in the emergency physician’s (EP) armamentarium for managing difficult airways.
METHODS
Study Design
This was a prospective experiment utilizing a human cadaveric model. The study was approved by the institutional review board of the hosting institution. Participants were fourth-year medical students entering emergency medicine (EM) residencies, EM residents, and attending physicians, who were all participants in or faculty of a residency-based emergency airway course, which included a cadaver laboratory practical session. The residency was a PGY1-3 EM residency, based at a suburban, academic community hospital.
Airway laboratory participants received a didactic lecture on the use of the ETTI, LMA, and other airway adjuncts. Those who wished to participate in this study were presented the clinical scenario of a patient with a difficult airway, and the need for endotracheal intubation was described. They were instructed in the technique of passing an ETTI through the LMA as described previously.1 Six unembalmed human cadavers were used for the experiment. Participants placed a size 4, classic LMA (The Laryngeal Mask Company Ltd., San Diego, CA), and inflated the LMA cuff, in the usual fashion, to obtain proper seating of the LMA. Seating was determined solely by watching the LMA rise into position when the cuff was inflated and was not confirmed with fiberoptics. Participants made no attempt to ventilate the cadaver through the LMA. They then attempted to pass a lubricated, 15 Fr, 60 cm, coude-tipped, reusable ETTI (Portex, Smiths Medical, Keene, NH) through the airspace/handle of the inflated LMA. Participants then deflated and removed the LMA while holding the ETTI in place by hand. An investigator then determined the location of the ETTI (trachea vs esophagus) using direct laryngoscopy and recorded the results on a data collection form. Procedural performance times were not limited or recorded in this experiment.
Data Analysis
The only recorded outcome was whether each placement of the ETTI was tracheal or esophageal. Independent variables recorded for each attempt included operator (with level of training) and cadaver. We input into a Microsoft Office Excel 2003 SP-2 spreadsheet (Microsoft Corp., Redmond, WA) and performed descriptive statistics. Ninety-five percent confidence intervals were computed using the Wald equation.
RESULTS
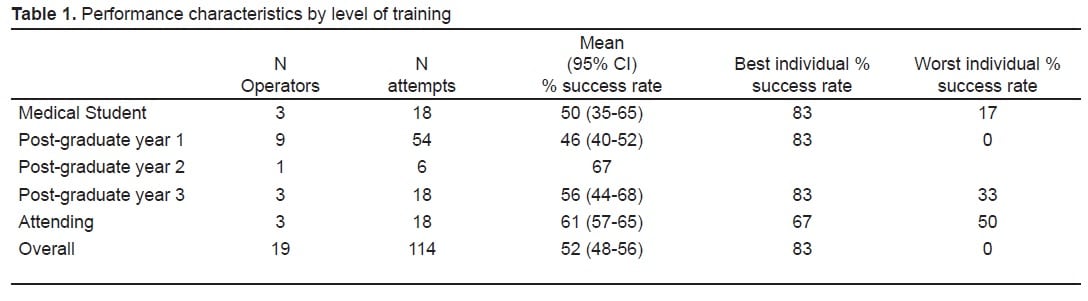
Nineteen residents and staff performed the procedure on each of six cadavers for a total of 114 attempts at the airway technique. Successful tracheal placement of the bougie stylet was achieved in 59 of the 114 attempts, for a total overall success rate of 52% (95% CI 48–56%). Success rates were not predicted by level of training of participants; however, individual success rates varied from 0% (one operator) to 83% (three operators). Success rates varied on individual cadavers from a low of 21% to a high of 79%. The test characteristics by level of experience of operator and by cadaver are presented in Tables 1 and and 2.

On post-trial inspection of the cadavers, two were noted to have distorted laryngo-tracheal anatomy, such that successful seating of the chosen LMA was deemed unlikely. These two cadavers had significantly lower rates of successful tracheal stylet placement. Eliminating them from the analysis increased the overall success rate to 63%.
DISCUSSION
In the management of the difficult airway, many adjuncts are available. The LMA is gaining popularity as a means of field airway management and rescue airway management in the ED; however most patients with an LMA will require eventual endotracheal intubation. Our study suggests that in patients with an LMA, a tracheal tube introducer may be passed through the LMA into the trachea 50–60% of the time, thus facilitating placement of an endotracheal tube.
There have been a number of reports in the anesthesia literature on the use of the ETTI as a bridge between the LMA and endotracheal intubation. Chadd et al.3 first described the technique of placing an ETTI through an LMA in two patients with known difficult airways. Both attempts were successful and were confirmed with fiberoptic laryngoscopy prior to placement of the endotracheal tube. Another study by Allison et al.4 used the same technique on 25 live patients in the operating room and reported an 88% success rate for correct tracheal placement. This study used fiberoptic laryngoscopy to confirm adequate LMA placement prior to placement of the ETTI, and again used fiberoptic laryngoscopy to confirm the location of the ETTI prior to endotracheal tube placement. They noted that the four failures occurred in patients with fiberoptically confirmed poor LMA placement. A larger study by Gabbott and Sasada5 used the same technique in simulated emergency airway conditions by applying cricoid pressure and manual in-line stabilization to 40 adult ASA 1 or 2 patients undergoing elective surgery requiring general anesthesia. With manual in-line stabilization and cricoid pressure the authors found the bougie entered the trachea in only nine of 40 patients (23%). They also performed the procedure in the standard fashion, without emergency precautions, and found the bougie entered the trachea in only 11 of 40 patients. Ahmed et al6 attempted to study the effect of head position on the technique in 20 patients undergoing elective surgery. They reported a success rate of 20% when patients were in the standard intubating position, and 0% when patients were in the neutral position.
Early studies reported very high rates of tracheal passage using this technique, while more recent studies have failed to achieve similar success rates. Our success rate is not surprising given the data already present.
We feel that the success of this procedure is facilitated by a number of variables. First, the LMA must be properly seated to ventilate the patient. In patients with distorted airway anatomy, and in those whom proper seating and ventilation are not possible, it is less likely that bougie stylet passage through the LMA will result in tracheal placement. This conclusion is supported by other literature.4,6 We also observed during the course of the experiment that the procedure was facilitated through maneuvering of the coude-tip of the stylet. Initially the stylet is more easily advanced through the LMA if the angle of the tip follows the angle of the LMA handle and points anteriorly. Once the stylet has passed the angle of the LMA handle and is passing beyond the LMA into the trachea, we found that spinning the stylet 180 degrees so that the coude-tip points inferiorly, along the patient’s trachea, allows a smoother passage into the trachea. Allsion and McCrory4specifically used this technique and achieved high success rates, while later studies5,6 failed to use this technique and report much lower numbers. We did not inform participants of this technique or control for its use, but we did note that participants who used this rotational technique of their own volition seemed to achieve higher rates of successful tracheal placement. This rotational technique perhaps contributed to our success rates midway between those of Allison and McCrory and later studies. We had very little difficulty in removing the LMA while maintaining the position of the bougie stylet. It is uncertain whether the sole participant who was successful on 0% of his or her attempts in our study used the rotational technique or not. In future investigations it would be helpful to standardize the use of the rotational technique, to ensure uniform optimization of the procedure.
This study also did not include blind methods of determining ETTI placement, or opportunities for operators to reposition and reattempt insertion, in its methodology. An ETTI’s location in the trachea is classically confirmed after blind placement by tactile stimuli, including “clicks” of the ETTI deflecting off the tracheal cartilage rings, and “hold up”, when forward advancement of the ETTI is halted at the carina.7 Were tactile confirmation and reattempts allowed, a higher ultimate success rate potentially could have been achieved.
LIMITATIONS
As this trial was performed on fresh frozen cadavers, the responsiveness of cadaveric tissue to this technique of rescue intubation may be different from that of live tissue. Thus, as with any cadaveric study, our findings may not generalize to clinical practice.
In addition, the study was performed after numerous attempts at direct laryngoscopic intubation during the course of an airway lab. It was already noted that the laryngeal tissue in two cadavers had significant trauma and distortion, making proper LMA placement unlikely. It is possible that the other cadavers had some occult distortion of their anatomy that was not recognized and thus contributed to poor placement of the LMA.
CONCLUSION
Overall, use of this technique could successfully bridge between an LMA and endotracheal intubation 50–60% of the time. However, manipulation of the ETTI could result in higher rates of success.
Footnotes
Supervising Section Editor: Tareg Bey, MD
Submission history: Submitted January 13, 2009; Revision Received April 16, 2009; Accepted May 21, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Joel A. Miller, MD, Department of Emergency Medicine, Darnall Army Medical Center, 36000 Darnall Loop Box 32, Ft. Hood, TX 76544
Email: joel.a.miller@us.army.mil
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Murdoch JAC. Emergency tracheal intubation using a gum elastic bougie through a laryngeal mask airway. Anaesthesia. 2005;60:626–7. [PubMed]
2. El-Orbany MI, Salem MR, Joseph NJ. The Eschmann tracheal tube introducer is not gum, elastic, or a bougie. Anesthesiology. 2004;101:1240. [PubMed]
3. Chadd GD, Ackers JW, Bailey PM. Difficult intubation aided by the laryngeal mask airway.Anaesthesia. 1989;44:1015. [PubMed]
4. Allison A, McCrory J. Tracheal placement of a gum elastic bougie using the laryngeal mask airway.Anaesthesia. 1990;45:419–20. [PubMed]
5. Gabbott DA, Sasada MP. Tracheal intubation through the laryngeal mask using a gum elastic bougie in the presence of circoid pressure and manual in-line stabilization of the neck. Anaesthesia.1996;51:389–90. [PubMed]
6. Ahmed AB, Nathanson MH, Gajraj NM. Tracheal intubation through the laryngeal mask airway using a gum elastic bougie: the effect of head position. J Clin Anesth. 2001;13:427–9. [PubMed]
7. Steinfeldt J, Bey T, Rich JM. Use of a Gum Elastic Bougie (GEB) in a zone II penetrating neck trauma. J Emerg Med. 2003;24:267–70. [PubMed]