
{kind=link}
| Author | Affiliation |
|---|---|
| Katherine W. D. Dolbec | University of Vermont College of Medicine, Burlington, VT Maine Medical Center, Department of Emergency Medicine, Portland, ME |
| George L. Higgins, III, MD | University of Vermont College of Medicine, Burlington, VT Maine Medical Center, Department of Emergency Medicine, Portland, ME |
| John R. Saucier, MD | University of Vermont College of Medicine, Burlington, VT Maine Medical Center, Department of Emergency Medicine, Portland, ME |
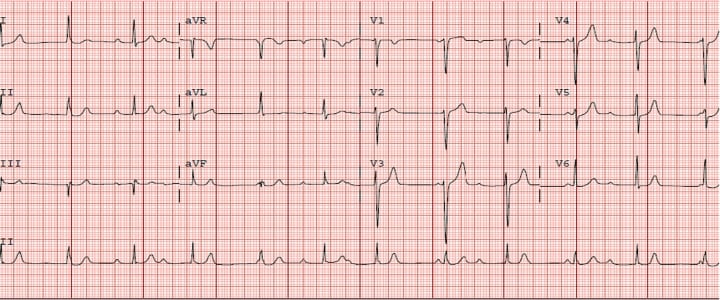
A healthy 37-year-old man presented to the emergency department complaining of 11 days of myalgias, fatigue, lightheadedness and rash. He was afebrile and hemodynamically stable. Scattered eythematous plaques on his trunk and extremities were consistent with erythema migrans (Figures 1). An electrocardiogram revealed complete heart block (Figure 2). His heart block persisted for 48 hours, fluctuating between third-degree and Mobitz type 1 and 2 second-degree atrioventricular (AV) block. Western Blot confirmed Lyme disease (LD), and IgM antibody levels suggested early disease.

In the United States, up to 10% of patients with untreated LD develop cardiac sequelae. These complications generally present during the early disseminated phase of illness, 1 to 6 weeks after the erythema migrans rash appears. Conduction disturbances predominate, most commonly complete heart block.1 The degree of block can fluctuate rapidly, usually progressing from high-level AV block through second-degree to first-degree heart block before complete resolution.2 The AV node is most commonly involved, but any level of the conduction system can be affected. Clinical heart failure is observed in approximately 10% of patients, and dilated cardiomyopathy can be a long-term consequence of untreated Lyme carditis.1 Other stigmata of carditis include diffuse T-wave flattening or inversion, ST-segment depression, decreased left ventricular function, and atrial and non-sustained ventricular tachyarrhythmias.2,3 A single case report describes valvular destruction.3The prognosis LD is excellent. Complete heart block generally resolves within one week, and lesser conduction abnormalities usually normalize within six weeks. Early antibiotic treatment appears to prevent cardiac involvement but does not hasten recovery once cardiac symptoms are manifest.1Patients with hemodynamic instability sometimes require temporary pacemaker placement.2
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted December 14, 2009; Revision Received February 2, 2010; Accepted December 29, 2009
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: George L. Higgins III, MD, Maine Medical Center, Department of Emergency Medicine, 47 Bramhall St, Portland, ME 04102
Email: higgig@mmc.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Pinto DS. Cardiac Manifestations of Lyme Disease. Medical Clinics of North Am. 2002;86:2.
2. McAlister HF, Klementowicz PT, Andrews C, et al. Lyme Carditis: An Important Cause of Reversible Heart Block. Ann of Internal Med. 1989;110(5):339–45. [PubMed]
3. Canver CC, Chanda J, DeBellis DM, et al. Possible Relationship Between Degenerative Cardiac Valvular Pathology and Lyme Disease. Ann of Thor Surg. 2000;70:283–285.