Volume 16, Issue 7, December 2015.
Brian J. Wolk, MD
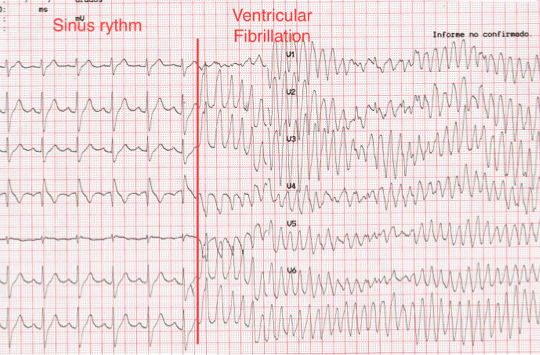
A 66-year-old female was transferred from an outside
hospital for possible ST segment elevation myocardial
infarction (STEMI). The patient reported feeling poorly for the
last day, with epigastric pain, nausea, and multiple episodes
of vomiting. Patient’s medical history was significant for
diabetes mellitus, hypertension, atrial fibrillation, and multiple
sclerosis. Electrocardiogram (EKG) was as noted (Figure).
Initial troponin was 0.14 (<0.03ng/mL). The patient was
taken emergently to the cardiac cath lab for possible posterior
STEMI. Angiogram demonstrated no significant evidence of
coronary artery disease, with an EF of 75%.
Volume 16, Issue 7, December 2015.
Lauren M. Porter, DO, et al.
A 42-year-old male was assisted from a car in front
of our inner city stand-alone emergency department (ED)
with a stab wound to the right chest. He was confused and
bleeding; his past medical history was unknown. The patient
was diaphoretic, pale and confused with a large vertical stab
wound over his right chest with no other obvious injuries.
On initial exam in the outlying ED, his back was obscured
by blood. He was transferred to the trauma center where
during a full secondary survey a 2cm wound was located over
the patient’s lumbar spine. The patient was stabilized and
taken for imaging. No focused assessment with sonography
for trauma (FAST) was done at either site; however, the
FAST exam, which emphasizes the search for extraluminal
blood, would not have been expected to find a foreign body
Volume 16, Issue 7, December 2015.
Krystal Garcia, BS, et al.
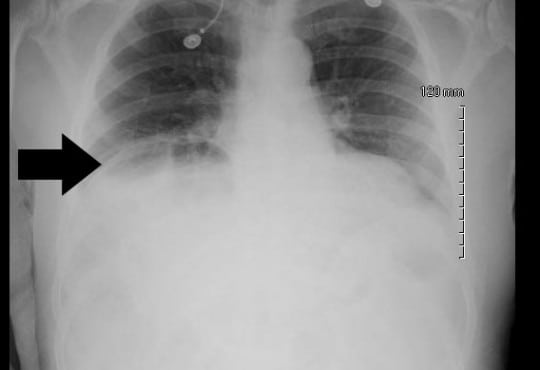
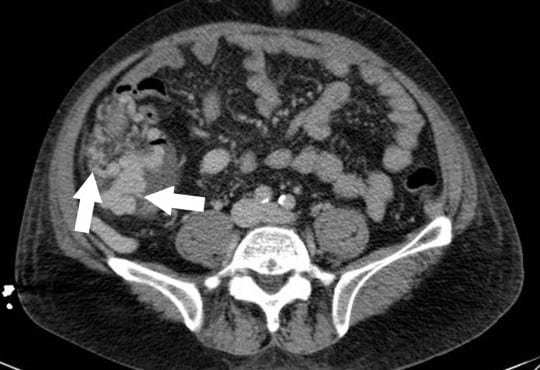
A 68-year-old male with a history of prostate cancer
presented with a two-day history of fever and left flank pain.
Vital signs included a temperature of 39.4 degrees Celsius with
93% oxygen saturation and heart rate of 112 beats per minute. An
upright chest radiograph showed concern for free intraperitoneal
air (Figure) with a white blood cell count of 17.3. A computed
tomography of the abdomen and pelvis revealed a Chilaiditi sign
with pyelonephritis, which was confirmed on urinalysis. He was
admitted for intravenous antibiotics.
Volume 16, Issue 7, December 2015.
Yudai Iwasaki, MD
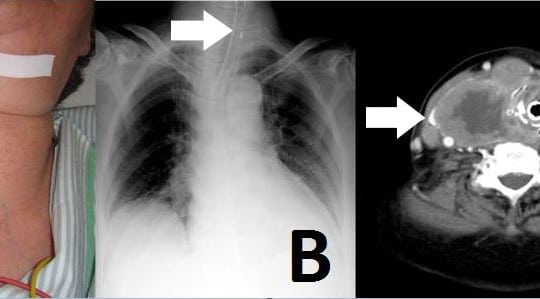
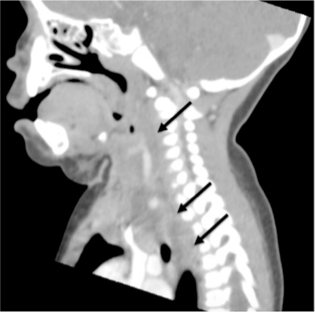
An 81-year-old woman was admitted to our emergency
department (ED) with neck swelling (Figure 1A) and
advancing dyspnea. Stridor was noted on auscultation of
her neck, and her breathing was labored. We immediately
diagnosed airway obstruction, and emergency intubation was
performed using a video laryngoscope (AWS-S100L®, Pentax
Corporation, Tokyo, Japan). The epiglottis was found to have
shifted to the left on chest video images and chest radiograph.
Volume 16, Issue 5, September 2015.
Thomas M. Nappe, Do, et al.
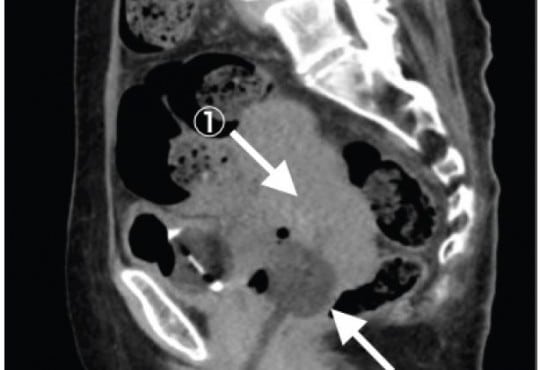
A 56-year-old female presented to the emergency
department (ED) with a chief complaint of urinary retention
and overflow incontinence for 24 hours, preceded by
progressive difficulty with voiding, worsening lower
abdominal discomfort and bloating. Her past medical
history was significant for small bowel obstruction and
neurofibromatosis with an associated benign pelvic tumor that
caused similar symptoms as a child, but had been known to
be stable since that time. She had also recently been treated
for a urinary tract infection. Her physical exam revealed
tachycardia and a diffusely tender abdomen with a palpable,
tender suprapubic mass extending just above her umbilicus.
Volume 16, Issue 5, September 2015.
William Mulkerin, MD, et al.
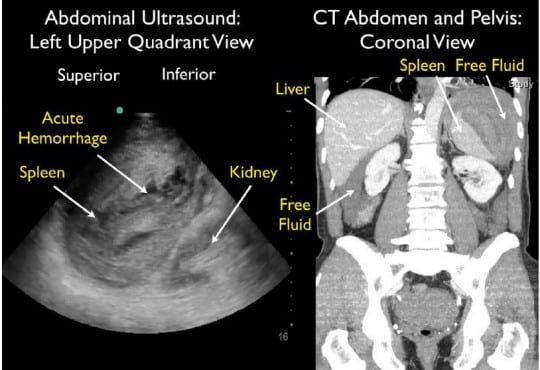
A 64-year-old male presented to the emergency
department (ED) with near syncope and worsening left flank
and shoulder pain. He had undergone a difficult colonoscopy
two days prior due to a tortuous colon. Initial vital signs
were normal. He looked uncomfortable and had significant
left upper quadrant abdominal tenderness with guarding.
Thirty minutes after ED arrival, his blood pressure dropped
to 73/59 mmHg, requiring aggressive fluid resuscitation.
Bedside focused assessment with sonography in trauma
(FAST) exam demonstrated free fluid in the abdomen with
mixed echogenicity of the spleen, suggestive of splenic injury.
Computed tomography (CT) demonstrated a large subcapsular
splenic hematoma with active extravasation and surrounding
intraperitoneal free fluid.
Volume 16, Issue 5, September 2015.
Jason D. Heiner, MD
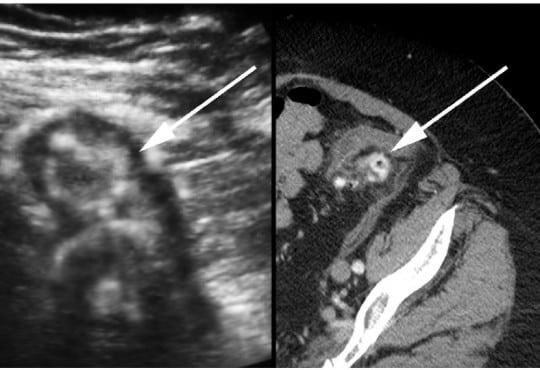
A 72-year-old otherwise healthy female presented to
the emergency department with two weeks of worsening
abdominal pain. She was afebrile with normal vital signs. Her
physical examination was notable for moderate abdominal
tenderness without rebound to the left and suprapubic
regions of the abdomen. Laboratory studies were remarkable
for a white blood cell count of 13,000/mm3
. A focused
bedside ultrasound over the patient’s region of maximal
discomfort revealed a thickened bowel wall and several
small contiguous hypoechoic projections surrounding a
hyperechoic center, suggestive of diverticulitis.
Volume 16, Issue 5, September 2015.
Caroline T. Brandon, MD, et al.
A 34-year-old male with diabetes presented to the
emergency department with four days of progressively
worsening redness, swelling and pain to his left buttock.
The patient denied fevers, chills, rectal pain or purulent
drainage from his rectum. His initial vital signs were heart
rate of 82; blood pressure of 146/92; and temperature of
98.2°F. The left buttock had a poorly circumscribed area of
induration; however, there was no fluctuance or crepitace.
Rectal exam was unremarkable. Because the patient’s
buttock pain was disproportionate to his exam findings,
a point-of-care ultrasound was performed to determine
if a more extensive process was present. The ultrasound
demonstrated cobblestoning, fascial thickening with edema,
and a large 4.5cm fluid collection extending and adjacent
to the rectum.
Volume 16, Issue 5, September 2015
Jill Tirabassi, MD, et al.
A 25-year-old male presented to the ski clinic after
colliding with a tree while snowboarding. He had immediate
sharp pain at his “tailbone,” but denied numbness and
weakness. Past medical history was initially reported as
unremarkable. On exam, he demonstrated midline tenderness
over the sacrum. Pelvic radiography was performed (Figure).
Volume 16, Issue 5, September 2015
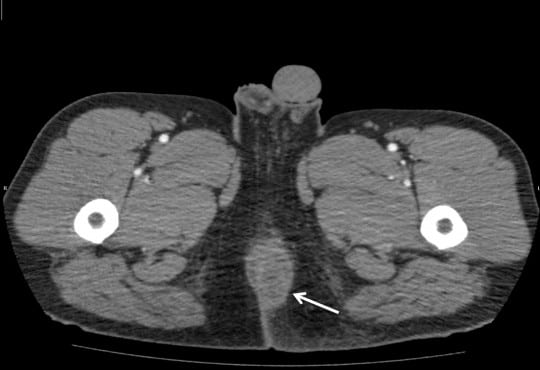
Jagdipak Heer, MD, et al.
A 31-year-old gravida 3 Para 3 female with no past
medical history, presented to the emergency department
complaining of a painless “boil” to the right groin, which
had been enlarging for over two months. Although it
was generally painless, she did suffer mild dyspareunia
at times. Antibiotics prescribed by her primary doctor
failed to resolve this mass so she decided to present to the
emergency department.
Volume 16, Issue 5, September 2015.
Stephen L. Thornton, MD, et al.
A previously healthy two-year-old boy presented to the
emergency department with vomiting. He was cyanotic with
mottling of both lower extremities. He was in respiratory
distress with retractions and diminished breath sounds. His
abdomen was distended and rigid. He had a pulse of 170 beats
per minute, blood pressure of 144/69mmHg and respiratory
rate of 42 breaths per minute. He was endotracheally
intubated. Chest and abdominal radiographs demonstrated a
tension pneumoperitoneum.
Volume 16, Issue 5, September 2015.
Tomohiro Sonoo, MD, et al.
A 67-year-old woman complaining of continuous fresh
vaginal hemorrhage came to our emergency department in a
pre-shock state. Examinations revealed an irregularly shaped
mass in the uterus and active arterial bleeding. Emergent
hysterectomy and interventional radiology were not
immediately available. Foley catheter with 20mL water was
inserted into the uterine cavity, then the balloon was pulled
to obstruct the uterus output (Figure). Her vital signs became
stabilized, and she was transferred to another hospital two
days later.
Volume 16, Issue 4, July 2015.
Patrick Burns, MD, et al.
A 48-year-old male presented with body aches and a chronic rash. He had no medical history aside from two unsuccessful treatments for presumed scabies and a recent diagnosis of psoriasis. Physical exam revealed hypotension, tachycardia, and profound, diffuse yellow crusting of the skin with erythematous erosions covering non-crusted areas. The patient was resuscitated and treated for septic shock while microscopic evaluation of scrapings of the crusted skin was performed.
Volume 16, Issue 4, July 2015.
Nobuhiko Kimura, MD, et al.
A 30-year-old man presented to the emergency department
for two weeks of diffuse abdominal pain and an episode of
emesis. He denied fever, prior surgery, or any other illnesses.
The patient reported going on a “crash diet regimen” one
month prior, resulting in an intentional weight loss of 25lbs in
30 days.
A 26-year-old female presented to the emergency department with a chief complaint of dizziness. Further history revealed that she was experiencing generalized weakness and intractable vomiting for three days, without complaint of abdominal pain or lower gastrointestinal symptoms. Physical examination uncovered mild dehydration with stable vital signs and non-fatigable, horizontal nystagmus consistent with internuclear opthalmoplegia.
Volume 16, Issue 4, July 2015.
Christian, MD, et al.
A 54-year-old man with a history of alcohol use presented with hematochezia and syncope. Upon arrival to the hospital, his bleeding had stopped. He was hemodynamically stable with hemoglobin of 11g/dL, international normalized ratio of 1.8 and platelets of 37K/mcL. Nasogastric aspirate found bilious gastric contents without blood.
Volume 16, Issue 4, July 2015.
Anderson, MD, et al.
A 68-day-old former 30-week infant presented with listlessness, apnea and bradycardia. The patient was intubated for airway protection. After intubation, breath sounds were auscultated bilaterally and a Pedi-Cap carbon dioxide detector had color change from purple to yellow. A nasogastric tube (NGT) was placed and a post-procedural chest radiograph was obtained.
Volume 16, Issue 3, May 2015
Rebekah Heckmann, MD, et al.
An 11-year-old healthy female presented to the emergency department with three days of worsening suprapubic pain, urinary retention, and constipation. She was afebrile with normal vital signs. Her physical examination was notable for suprapubic distention and bulging pink vaginal tissue at the introitus. Bedside ultrasound suggested a distended bladder.
Volume 16, Issue 3, May 2015
Kimberly Stillman, DO, et al.
A 76-year-old male presented to the emergency department complaining of intense abdominal pain. He reported one week earlier an upper respiratory illness with violent coughing spells. Past medical history included recent percutaneous coronary intervention for a myocardial infarction 6 months prior where he received three drug-eluting stents and was subsequently discharged home on Prasugrel (Effient) and Aspirin.
Volume 16, Issue 3, May 2015
Karim El-Kersh, MD, et al.
A 62-year-old man presented to the emergency department with hypotension and diarrhea secondary to Clostridium difficile infection. Due to poor peripheral access, a left internal jugular vein triple lumen central venous catheter (CVC) was inserted for fluid resuscitation. The CVC was placed under real-time ultrasound guidance, which revealed normal anatomy, with no resistance during placement.
Volume 16, Issue 3, May 2015
Kubwimana M. Mhayamaguru, MD, et al.
A 61-year-old female presented to the emergency department complaining of constipation and vaginal bulge with valsalva 89 days after a robotic-assisted hysterectomy. The patient had intercourse three days prior to presentation and experienced postcoital abdominal discomfort with vaginal bleeding. She denied any other trauma. She had no other complaints and denies fevers, chills, nausea, vomiting, abdominal distension, or constipation. Physical exam revealed exposed bowel protruding through the vaginal cavity.
Volume 16, Issue 3, May 2015
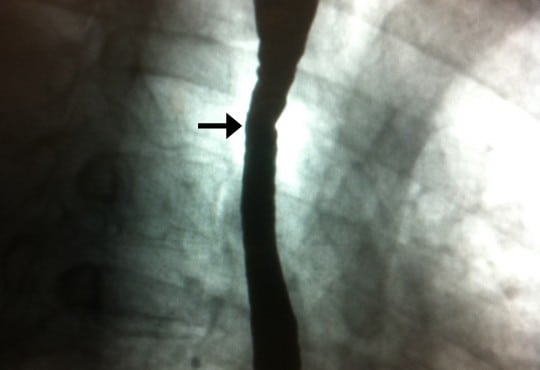
Demis N. Lipe, MD, MSc, et al.
A 42-year-old man with history of esophageal strictures and esophageal dilation presented to the emergency department with 12 hours of dysphagia and non-bloody emesis. His symptoms started upon waking and included sharp retrosternal pain during each attempt at swallowing. Dysphagia occurred with both solids and liquid. He denied difficulty initiating swallowing, pain with eating the previous night, halitosis and hematemesis.
Volume 16, Issue 2, March 2015
Alice Chao, MD et al.
An 86-year-old female was brought in by ambulance for severe abdominal and back pain. She was hypotensive en route and appeared to be in distress upon arrival to the emergency department. Her abdomen was tense and distended with diffuse tenderness to palpation present.
Volume 16, Issue 2, March 2015
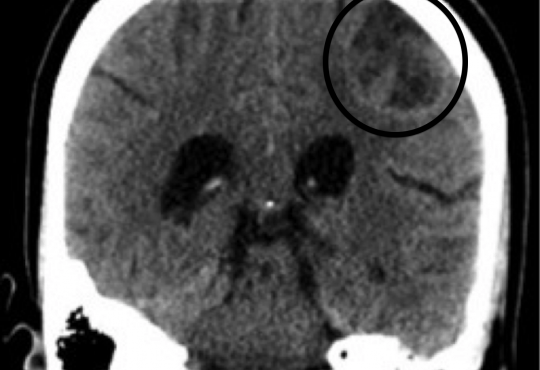
Pablo Aguilera, MD et al.
A 22-year-old healthy male university student presented to the emergency department (ED) complaining of syncope. He had five episodes of loss of consciousness from 10 to 40 seconds in length, with loss of postural tone and full recovery without intervention in the last month.
Volume 16, Issue 2, 2015
Michael Butterfield, MD et al.
A nine-month-old girl was brought to the emergency department because of right neck swelling. She had recently been discharged from the same hospital after a brief admission for pneumonia that had followed influenza.
Volume 16, Issue 2, March 2015
Thomas M. Nappe, DO et al.
An 18-year-old female presented to the emergency department with three days of worsening left flank pain. Past medical history included asymptomatic bacteriuria. She denied prior similar episodes or inciting events, and was currently being treated with trimethoprim sulfamethoxazole by an urgent care center for a urinary tract infection, although she denied having any urinary symptoms.
{kind=link}