
{kind=link}
| Author | Affiliation |
|---|---|
| Yudai Iwasaki, MD | Ohta Nishinouchi Hospital, Department of Critical Care and Emergency Medicine, Fukushima, Japan |
Case report
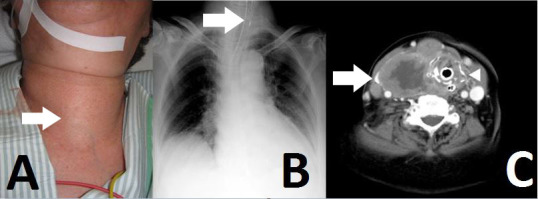
An 81-year-old woman was admitted to our emergency department (ED) with neck swelling (Figure 1A) and advancing dyspnea. Stridor was noted on auscultation of her neck, and her breathing was labored. We immediately diagnosed airway obstruction, and emergency intubation was performed using a video laryngoscope (AWS-S100L®, Pentax Corporation, Tokyo, Japan). The epiglottis was found to have shifted to the left on chest video images and chest radiograph (Figure 1B). After intubation, computed tomography and cervical ultrasonography were performed, and we noted swelling of the thyroid, which was superior to the right lobe, and tumor invasion into the trachea without lung metastases (Figure 1C). After admission, fine needle aspiration was performed, and she was diagnosed with undifferentiated carcinoma. We could not perform tracheostomy or place an intratracheal stent because of continuous intratracheal bleeding and disseminated intravascular coagulation. The patient died 28 days after admission.
Discussion
Airway obstruction caused by thyroid carcinoma is rare.1,2 Lung metastases often are associated with respiratory symptoms and are the most fatal complication.3
When patients present to the ED with airway obstruction, physicians should consider acute epiglottitis, peritonsillar or retropharyngeal abscess, and foreign body aspiration as possible causes. Although invasion of thyroid carcinoma resulting in airway obstruction is rare, physicians should consider it an oncologic emergency. Visual examination, palpation, and auscultation of the neck can help in the differential diagnosis of airway obstruction.
Footnotes
Section Editor: Sean O. Henderson, MD
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Yudai Iwasaki, MD, Ohta Nishinouchi Hospital, Department of Critical Care and Emergency Medicine, Fukushima, Japan. Email: yudai.i0213@gmail.com. 12 / 2015; 16:1208 – 1209
Submission history: Revision received October 1, 2015; Accepted October 21, 2015
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Musa AA, Adebayo SB, Banjo AA, et al. Emergency partial thyroidectomy under cervical block to relieve severe acute airway obstruction from thyroid cancer. Afr Health Sci. 2008;8(3):186-189.
2. Lui JT, Khalil MN, Chandarana SP. Primary squamous cell of the thyroid–an abbreviated clinical presentation. J Otolaryngol Head Neck Surg. 2014;43:17.
3. Kitamura Y, Shimizu K, Nagahama M, et al. Immediate causes of death inthyroid carcinoma: clinicopathological analysis of 161 fatal cases. J Clin Endocrinol Metab. 1999;84(11):4043-9.