Volume 17, Issue 4, July 2016
Samuel Lam, MD, et al.
In recent years studies have been published on the use of beside ultrasound (BUS) to diagnose appendicitis in the emergency department (ED). Its popularity is likely due to the improving ultrasound skills of emergency physicians, as well as the obvious BUS advantages of no ionizing radiation emission, and ease of performance and interpretation at the bedside. Use of ultrasound in suspected appendicitis is also supported by American College of Radiology recommendations, especially in the pediatric population.
Volume 17, Issue 4, July 2016
Kelly Kesler, MD, et al.
A 29-year-old female with no significant past medical history presented with palpitations, nausea, diaphoresis and lightheadedness. Symptoms began 15 minutes prior to arrival. She reported several similar episodes previously that self-resolved within seconds, but had no previous medical evaluations for these symptoms. Initial vital signs were significant for blood pressure of 93/61, irregular heart rate between 180 and 200, respiratory rate of 18, and oxygen saturation of 99% on room air. Physical examination was otherwise unremarkable. The electrocardiogram (ECG) is shown in Figure 1. This was interpreted as atrial fibrillation with rapid ventricular rate, and the patient was treated with rate control with no effect. The patient later spontaneously converted to normal sinus rhythm and repeat ECG was notable for delta waves concerning for Wolff-Parkinson-White Syndrome (WPW) as seen in Figure 2. She was admitted to cardiology for cardiac ablation.
Volume 17, Issue 4, June 2016
Zachary Dezman, MD, MS, et al.
A sexually active 35-year old woman presented to the emergency department with intermittent vaginal spotting and pelvic cramping over the preceding four weeks. She had an intrauterine device (IUD) placed three months prior and has never been pregnant. The threads of the IUD and a small amount of blood coming from the cervix were seen on pelvic exam. Laboratory testing revealed a β-human chorionic gonadotropin level of 70,000 mIU/mL. Pelvic ultrasound imaging showed the IUD and a viable intrauterine pregnancy.
Author Affiliation Charles W. Bugg, MD, PhD Keck School of Medicine, LAC+USC Medical Center, Department of Emergency Medicine, Los Angeles, California Kristin Berona, MD Keck School of Medicine, LAC+USC Medical Center, Department of Emergency Medicine, Los Angeles, California Supplementary information A 56-year-old male presented to the emergency department (ED) with fatigue, generalized weakness, cough without […]
Volume 17, Issue 2, March 2016.
Timothy D. Roberts, MBChB
An eight-year-old boy presented to the emergency
department (ED) with a 2cm-long laceration over the
prepatellar region of his left knee after falling over and
cutting his knee on broken glass. Physical examination
demonstrated the laceration breached the dermis but
otherwise there was no obvious defect in the deep fascial
layer.
Volume 17, Issue 2, March 2016.
Kristin H. Dwyer, MD, MPH, et al.
A 26-year-old female presented to the emergency
department with three days of subjective fevers, dry cough
and pleuritic chest discomfort. On exam, her vital signs
were significant for a heart rate of 106/minute and oxygen
saturation of 95% on room air. Her lung exam revealed
decreased breath sounds at the right base. A bedside lung
ultrasound and a chest radiograph were performed.
Volume 17, Issue 2, March 2016.
Meina J. Michael, BS, et al.
A 63-year-old female with insulin-dependent type II
diabetes mellitus and end-stage renal disease presented to the
emergency department with spontaneous blistering to the tips
of her left index and middle fingers. The blisters had gradually
become tense and mildly painful over the preceding 10 days.
She denied burn injury, trauma, fever, or new medications.
On physical exam, the patient was noted to have a tense,
nontender bullae on the pad of the left middle finger, and a
collapsed, hemorrhagic bullae on the left index finger. There
were no signs of inflammation or infection. A radiograph of
the left hand, complete blood count, and basic metabolic panel
were unremarkable. The diagnosis of bullosis diabeticorum
was made, and supported by a consulting endocrinologist.
Volume 17, Issue 2, March 2016.
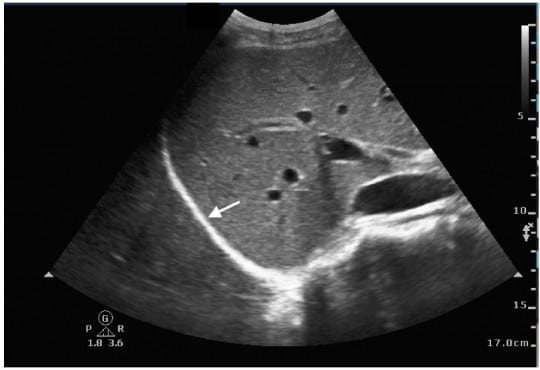
Samuel L. Burleson, MD, et al.
A 58-year-old female with a past medical history of
hepatitis C virus-induced cirrhosis presented to the emergency
department with three days of increasing abdominal pain,
chills, and nausea and vomiting. Abdominal physical
examination revealed gross ascites with fluid wave. Diagnostic
paracentesis resulted in the aspiration of approximately 60mL
of white turbid peritoneal fluid (Figure).
Volume 17, Issue 2, March 2016.
Michael T. Long, MD
A 16-year-old male presented with three months of
palpitations at rest, fatigue, and episodic pre-syncope; his
paternal grandfather died following presumed premature
myocardial infarction at age 30. He was seen and discharged
one week previously at an outside emergency department
(ED). He followed up with his pediatrician and was promptly
referred to our pediatric ED for evaluation given his risk factors.
Pertinent vitals on arrival were pulse 110, blood pressure
129/66, and oxygen saturation 97% on room air. His exam
was remarkable for a left upper sternal border 2/6 holosystolic
murmur with radiation to apex. In addition, the patient had a
chest radiograph (Figure), a nonspecific but abnormal EKG, and
a point-of-care ultrasound (POCUS) of the heart performed.
Volume 17, Issue 1, January 2016.
Adam Janicki, MD, et al.
A 64-year-old woman presented to the emergency department
after falling when she tripped on a rock while doing yard work.
Physical examination revealed an open deformity of the left
forearm (Figure 1). Radial pulse was palpable, sensation was
intact, and she had normal range of motion of the fingers. While
awaiting radiographs, bedside ultrasound was performed (Video).
Ultrasound revealed intact radius and ulna and a large linear
foreign body. The wooden foreign body was removed at the
bedside (Figure 2) and patient was admitted for observation and
intravenous antibiotics.
Volume 17, Issue 1, January 2016.
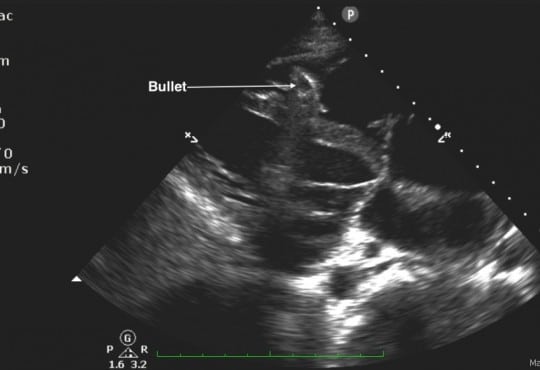
Abdullah Bakhsh, MD, et al.
A 25-year-old male was brought in by ambulance to
the emergency department (ED) after sustaining a gunshot
wound to his chin and left shoulder. Upon arrival to the
ED, his airway was intact without evidence of blood in the
oropharynx. He was found to have slightly diminished breath
sounds on the left side, with respirations at 34 breaths per
minute, a blood pressure of 72/50mmHg, and a heart rate of
76 beats per minute with cool extremities and poor peripheral
pulses. His focused abdominal sonography in trauma exam
showed a foreign body within the right ventricle without a
pericardial effusion (Figure 1 and Video). An upright portable
chest radiograph performed immediately thereafter showed
blunting of the left costophrenic angle with a bullet fragment
overlying the cardiac shadow (Figure 2).
Volume 17, Issue 1, January 2016.
Rohat Ak, MD, et al.
A 45-year-old man presented with headache for two days.
He described the quality of headache as throbbing, and it was
unilateral. There was no history of fever, vomiting, blurred
vision, ear discharge or trauma, no relevant past medical or
drug history and no family history of note. On examination,
he was afebrile with pulse 76/min, regular, blood pressure of
130/80mmHg. His pupils and speech appeared normal. There
were no papilledema, sensory deficit, focal neurological deficit
or signs of meningeal irritation. Hyperdensity of right transverse
sinus (Figure 1) and superior sagittal sinus was identified on
unenhanced computed tomography (CT). Magnetic resonance
venography (MRV) demonstrated lack of flow in right transverse
sinus (Figure 2) and superior sagittal sinus.
Volume 16, Issue 7, December 2015.
Warren Wiechmann, MD
As hospitals across the nation were preparing for the
possibility of Ebola or Middle Eastern respiratory syndrome
(MERS-CoV) cases, healthcare workers underwent intricate
training in the use of personal protective equipment (PPE).
An Ebola or MERS-CoV patient requiring intubation places
a healthcare worker at risk for exposure to bodily secretions.
The procedure must be performed only after appropriate
PPE is donned.1
Intubating while wearing PPE is yet another
challenge identified in caring for these patients. Manual
dexterity and free movement decreases when wearing PPE,
and may increase length of time to successful intubation.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 61-year-old female was brought in by ambulance after
being the restrained driver of a head-on motor vehicle collision
at 40MPH. There was positive airbag deployment and intrusion
from the other vehicle. During workup, the patient complained
of midline chest pain, and left chest wall pain. The patient
was not in acute respiratory distress, and had the following
vital signs: temperature 37°C, heart rate 84, blood pressure
of 150/64, respiratory rate 18, and oxygen saturation of 97%
on two liters of oxygen. On physical exam, breath sounds
were heard bilaterally, with no acute cardiopulmonary issues
identified. A bruise was identified on the lower abdomen,
which was thought to be a potential seatbelt sign. A focused
assessment with sonography for trauma was negative, and an
ultrasound of additional chest and mediastinal structures was
performed for the chest tenderness.
Volume 16, Issue 7, December 2015.
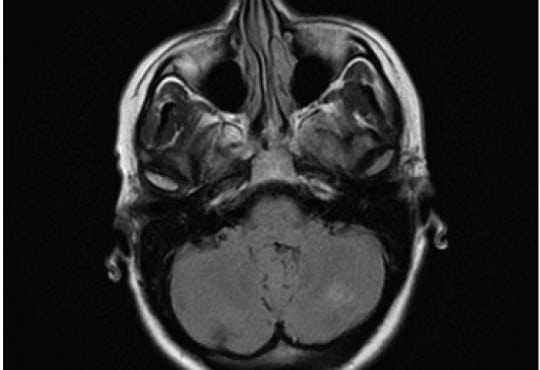
Tara Murphy, et al.
Posterior reversible encephalopathy syndrome (PRES) is an unusual condition typified by acute
visual impairment caused by sudden, marked parieto-occipital vasogenic edema. Thought to be
inflammatory in origin, it has been described in patients undergoing chemotherapy, with autoimmune
disease, and in some infections. We report a case of PRES that occurred one week after an episode
of acute pancreatitis in an otherwise healthy 40-year-old female. There was progressive visual
impairment over a 24-hour period with almost complete visual loss, with characteristic findings on
magnetic resonance imaging. After treatment with steroids, the visual loss recovered. Clinicians
should retain an index of suspicion of this rare condition in patients with visual impairment after acute
pancreatitis.
Volume 16, Issue 7, December 2015.
Jesse Z. Kellar, MD, et al.
A 14-year-old African American male presented to the emergency department with worsening left
eye redness, swelling, and vision loss over the preceding three days. History was notable for similar
eye redness and swelling without vision loss four months earlier, which improved following a brief
course of prednisone. He endorsed mild eye irritation and tearing with bright lights. There was
no history of fever, respiratory symptoms or trauma. Mother was medicating patient with leftover
antibiotic eye drops x3 days without improvement. Physical examination on presentation notable
for proptosis of left eye, lid, and periorbital swelling, mild scleral injection, and central vision loss in
affected eye (20/200 OS, 20/25 OD). Extraocular movements and pupillary exam were normal. No
corneal fluorescein uptake, abnormal cell, flare, or siedel sign were seen during slit lamp exam. Eye
pressures were 24 mmHg in both eyes. Bedside ultrasonography was performed (Figure 1 showing
retinal detachment, Ultrasound Video 2 showing detachment in orbital scan).
Volume 16, Issue 7, December 2015.
Erik A. Berg, MD
A 60-year-old female with a history of
ventriculoperitoneal shunt (VPS) placement three years
prior presented with a painful abdominal wall mass.
The patient denied fevers, nausea, vomiting, headaches,
or dizziness. Physical exam revealed an afebrile, wellappearing
female with a raised, erythematous, fluctuant mass
on the right lower abdominal wall. She had no abdominal
tenderness otherwise. Labs were unremarkable. A bedside
ultrasound revealed a complex fluid collection over the
area of fluctuance that tracked along the course of the VPS
tubing into the abdomen. Plan for incision and drainage was
deferred. Neurosurgery was consulted. The neurosurgeon
attempted to tap the shunt but encountered very high
resistance. The patient was admitted for intravenous antibiotics for VPS infection and malfunction.
Volume 16, Issue 7, December 2015.
Sean P. Nordt, MD, PharmD, et al.
A 37-year-old male presented to the emergency
department (ED) in police custody for “medical clearance”
before being taken to jail. The patient was approached by
police officers for suspicion of selling illicit drugs. When
approached by police he ran away and was witnessed to
swallow several small plastic baggies suspected to contain
heroin. He was apprehended and brought to the ED.
On arrival, he was asymptomatic with a blood pressure
144/83mmHg, heart rate 67bpm, respiratory rate of 19bpm,
oxygen saturation of 99% on room air and afebrile. A Glasgow
coma score was 15 and he was alert and oriented to person,
place and time. Patient had a negative review of systems.
On physical examination pupils were 4mm and reactive to
light, lungs clear to auscultation and had normal respiratory
rate with normal cardiovascular exam. Abdomen was soft,
non-tender and non-distended with present bowel sounds.
The patient admitted to ingesting approximately 20 packets
of heroin to avoid being charged with possession. The patient
declined activated charcoal and whole bowel irrigation (WBI)
with polyethylene glycol-electrolyte solution (PEG-ELS). The
patient declined a urine toxicology immunoassay screen. A
computed tomography (CT) of his abdomen with contrast was
obtained and read as normal except for a cluster of foreign
bodies within the distal stomach likely contained within a
plastic bag.
Volume 16, Issue 7, December 2015.
Po-Jen Yang, MD, et al.
A previously healthy 27-year-old man presented to the
emergency department with a three-day history of left lower
quadrant pain. He denied fever, nausea, vomiting, or diarrhea.
Vital signs were unremarkable, and physical examination
revealed tenderness in the left iliac fossa without peritoneal
signs. His leukocyte count and C-reactive protein were slightly
elevated. On abdominal computed tomography (CT) (Figure),
a fatty ovoid mass abutting sigmoid colon demonstrated the
infarcted or inflamed appendix epiploica. A surrounding
hyperdense rim (hyperattenuating ring sign) represented the
inflamed visceral peritoneal covering, and the central linear
hyperdensity corresponded to the thrombosed central vessel.
Volume 16, Issue 7, December 2015.
Jonathan G. Wagner, MD, et al.
A 52-year-old African American male with a long history of poorly controlled hypertension presented
to the emergency department (ED) with two days of genital edema and pain. During ED work-up,
the patient developed sudden onset of non-pitting, non-pruritic, and non-urticarial upper lip edema.
Review of his antihypertensive medication list revealed that he normally took benazepril, highly
suggestive of a diagnosis of angiotensin-converting-enzyme inhibitor-related angioedema (ACEIRA).
We present the first reported case of penile ACEI-RA that progressed to involve the oropharynx.
The ED management of the condition and some of the newer treatment options available for ACEIRA
is also briefly discussed.
Volume 16, Issue 7, December 2015.
Leonieke Groot, MD, et al.
Introduction: Currently, it is common practice in the emergency department (ED) for pain relief
in hip-fracture patients to administer pain medication, commonly systemic opioids. However, with
these pain medications come a high risk of side effects, especially in elderly patients. This study
investigated the safety profile and success rate of fascia iliaca compartment block (FICB) in a
busy ED. This ED was staffed with emergency physicians (EPs) and residents of varying levels of
experience. This study followed patients’ pain levels at various hourly intervals up to eight hours
post procedure.
Methods: Between September 2012 and July 2013, we performed a prospective pilot study on
hip-fracture patients who were admitted to the ED of a teaching hospital in the Netherlands. These
patients were followed and evaluated post FICB for pain relief. Secondary outcome was the use of
opioids as rescue medication.
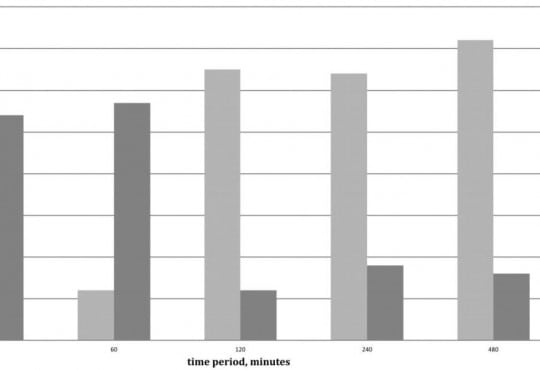
Results: Of the 43 patients in this study, patients overall experienced less pain after the FICB
(p=0.04). This reduction in pain was studied in conjunction with the use and non-use of opioids. A
clinically meaningful decrease in pain was achieved after 30 minutes in 62% of patients (54% with
the use of opioids, 8% without opioids); after 240 minutes in 82% of patients (18% with opioids, 64%
without opioids); after 480 minutes in 88% of patients (16% with opioids, 72% without opioids). No
adverse events were reported.
Conclusion: In a busy Dutch ED with rotating residents of varying levels of experience, FICB seems
to be an efficient, safe and practical method for pain reduction in patients with a hip fracture. Even
without the use of opioids, pain reduction was achieved in 64% of patients after four hours and in
72% of patients after eight hours.
Volume 16, Issue 7, December 2015.
Peter Moffett, MD, et al.
A 65-year-old male presented to the emergency department
complaining of two hours of severe lower abdominal
pain radiating into his left testicle. The patient described a
vascular procedure in the past but did not recall the details.
An emergent bedside ultrasound was performed to evaluate
the abdominal aorta. During the exam an echogenic object
consistent with a prior endovascular stent was discovered
in the distal aorta prompting further ultrasound evaluation
of the iliac artery (Figure). A true lumen (thin black arrow)
was visualized with evidence of leak (white arrows) during
color Doppler evaluation. The patient was taken emergently
to computed tomography and the diagnosis of an iliac artery
pseudoaneurysm from an endoleak was confirmed.
Volume 16, Issue 7, December 2015.
Brandon Fetterolf, DO, et al.
A 35-year-old male presented with lower gum
pain associated with fever, chills, and sore throat. His
medical history included intravenous drug use, human
immunodeficiency virus infection, and hepatitis C. Physical
exam revealed tachycardia, a temperature of 38.9°C, anterior
cervical lymphadenopathy, halitosis, an edematous lower lip,
and purulent ulcers anterior and posterior to lower central
incisors with marked tenderness and erythema (Figure).
His laboratory work was notable for a low white blood cell
count (2.6 thousand/µl), neutropenia (0.11 thousand/µl), a
low absolute CD4 lymphocyte count (0.5 thousand/µl), and
elevated C-reactive protein (129mg/L) and sedimentation
rate (23mm/hr). A computed tomography study showed a
0.5×1.3×0.3cm abscess anterior to the mandibular symphysis.
Volume 16, Issue 7, December 2015.
Sarah E. Frasure, MD, et al.
A 42-year-old female presented to the emergency
department with diffuse abdominal pain, vaginal discharge,
and a fever of 102°F. She described multiple recent male
sexual partners, with inconsistent condom use. Her vital
signs were unremarkable. Her physical exam was notable for
moderate right lower quadrant tenderness to palpation. There
was no cervical motion tenderness. The emergency physician
performed a bedside abdominal ultrasound (Video), and
subsequently ordered a computed tomography (Figure), which
confirmed the diagnosis.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 41-year-old female presented to the emergency
department with nausea, vomiting and foreign body sensation
in her throat. The patient had multiple co-morbidities including
hypertension, diabetes, cervical cancer and gastroparesis with
gastrojejunostomy (GJ) tube. The patient had stable vitals, was
in no respiratory distress, and her only complaint was mild throat
pain and abdominal pain at the GJ tube insertion site. Physical
exam revealed a foreign object in the oropharynx (Figure 1).
Abdominal exam showed a soft, non-distended, non-tender
abdomen with GJ-tube and colostomy in place. Abdominal series
and upright chest radiograph were obtained (Figure 2).
Volume 16, Issue 7, December 2015.
Marc A. Polacco, MD, et al.
Often discovered only after an extensive work up for hemoptysis and hematemesis, vallecular varices
are a rare cause of oral bleeding that increase patient morbidity due to delay of diagnosis.
We describe an 89-year-old male who presented with a week of intermittent oral blood production. A
vallecular varix was identified on fiberoptic laryngoscopy after studies for hematemesis and hemoptysis
had been performed, including negative esophagogastroduodenoscopy and bronchoscopy.
Awareness of this pathology and key points in the patient history can direct the clinician toward the
correct diagnosis, expediting treatment and limiting invasive diagnostic procedures for pulmonary or
gastric etiologies of bleeding.
{kind=link}