Volume 17, Issue 2, March 2016.
Meina J. Michael, BS, et al.
A 63-year-old female with insulin-dependent type II
diabetes mellitus and end-stage renal disease presented to the
emergency department with spontaneous blistering to the tips
of her left index and middle fingers. The blisters had gradually
become tense and mildly painful over the preceding 10 days.
She denied burn injury, trauma, fever, or new medications.
On physical exam, the patient was noted to have a tense,
nontender bullae on the pad of the left middle finger, and a
collapsed, hemorrhagic bullae on the left index finger. There
were no signs of inflammation or infection. A radiograph of
the left hand, complete blood count, and basic metabolic panel
were unremarkable. The diagnosis of bullosis diabeticorum
was made, and supported by a consulting endocrinologist.
Volume 17, Issue 2, March 2016.
Samuel L. Burleson, MD, et al.
A 58-year-old female with a past medical history of
hepatitis C virus-induced cirrhosis presented to the emergency
department with three days of increasing abdominal pain,
chills, and nausea and vomiting. Abdominal physical
examination revealed gross ascites with fluid wave. Diagnostic
paracentesis resulted in the aspiration of approximately 60mL
of white turbid peritoneal fluid (Figure).
Volume 17, Issue 2, March 2016.
Michael T. Long, MD
A 16-year-old male presented with three months of
palpitations at rest, fatigue, and episodic pre-syncope; his
paternal grandfather died following presumed premature
myocardial infarction at age 30. He was seen and discharged
one week previously at an outside emergency department
(ED). He followed up with his pediatrician and was promptly
referred to our pediatric ED for evaluation given his risk factors.
Pertinent vitals on arrival were pulse 110, blood pressure
129/66, and oxygen saturation 97% on room air. His exam
was remarkable for a left upper sternal border 2/6 holosystolic
murmur with radiation to apex. In addition, the patient had a
chest radiograph (Figure), a nonspecific but abnormal EKG, and
a point-of-care ultrasound (POCUS) of the heart performed.
Volume 17, Issue 1, January 2016.
Adam Janicki, MD, et al.
A 64-year-old woman presented to the emergency department
after falling when she tripped on a rock while doing yard work.
Physical examination revealed an open deformity of the left
forearm (Figure 1). Radial pulse was palpable, sensation was
intact, and she had normal range of motion of the fingers. While
awaiting radiographs, bedside ultrasound was performed (Video).
Ultrasound revealed intact radius and ulna and a large linear
foreign body. The wooden foreign body was removed at the
bedside (Figure 2) and patient was admitted for observation and
intravenous antibiotics.
Volume 17, Issue 1, January 2016.
Abdullah Bakhsh, MD, et al.
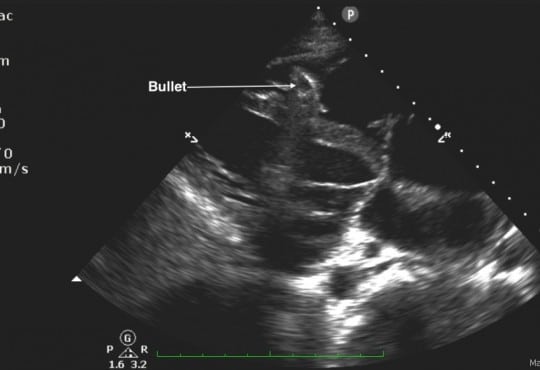
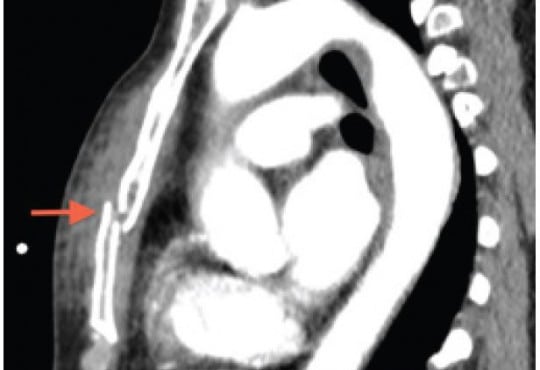
A 25-year-old male was brought in by ambulance to
the emergency department (ED) after sustaining a gunshot
wound to his chin and left shoulder. Upon arrival to the
ED, his airway was intact without evidence of blood in the
oropharynx. He was found to have slightly diminished breath
sounds on the left side, with respirations at 34 breaths per
minute, a blood pressure of 72/50mmHg, and a heart rate of
76 beats per minute with cool extremities and poor peripheral
pulses. His focused abdominal sonography in trauma exam
showed a foreign body within the right ventricle without a
pericardial effusion (Figure 1 and Video). An upright portable
chest radiograph performed immediately thereafter showed
blunting of the left costophrenic angle with a bullet fragment
overlying the cardiac shadow (Figure 2).
Volume 17, Issue 1, January 2016.
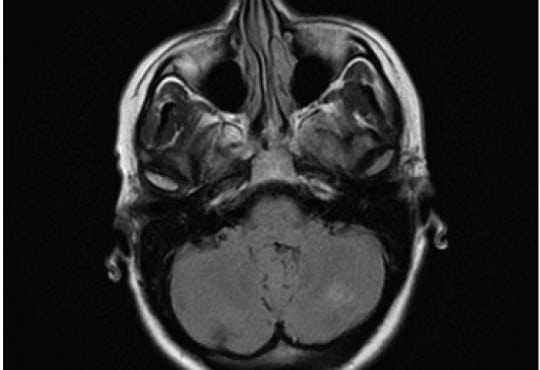
Rohat Ak, MD, et al.
A 45-year-old man presented with headache for two days.
He described the quality of headache as throbbing, and it was
unilateral. There was no history of fever, vomiting, blurred
vision, ear discharge or trauma, no relevant past medical or
drug history and no family history of note. On examination,
he was afebrile with pulse 76/min, regular, blood pressure of
130/80mmHg. His pupils and speech appeared normal. There
were no papilledema, sensory deficit, focal neurological deficit
or signs of meningeal irritation. Hyperdensity of right transverse
sinus (Figure 1) and superior sagittal sinus was identified on
unenhanced computed tomography (CT). Magnetic resonance
venography (MRV) demonstrated lack of flow in right transverse
sinus (Figure 2) and superior sagittal sinus.
Volume 16, Issue 7, December 2015.
Warren Wiechmann, MD
As hospitals across the nation were preparing for the
possibility of Ebola or Middle Eastern respiratory syndrome
(MERS-CoV) cases, healthcare workers underwent intricate
training in the use of personal protective equipment (PPE).
An Ebola or MERS-CoV patient requiring intubation places
a healthcare worker at risk for exposure to bodily secretions.
The procedure must be performed only after appropriate
PPE is donned.1
Intubating while wearing PPE is yet another
challenge identified in caring for these patients. Manual
dexterity and free movement decreases when wearing PPE,
and may increase length of time to successful intubation.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 61-year-old female was brought in by ambulance after
being the restrained driver of a head-on motor vehicle collision
at 40MPH. There was positive airbag deployment and intrusion
from the other vehicle. During workup, the patient complained
of midline chest pain, and left chest wall pain. The patient
was not in acute respiratory distress, and had the following
vital signs: temperature 37°C, heart rate 84, blood pressure
of 150/64, respiratory rate 18, and oxygen saturation of 97%
on two liters of oxygen. On physical exam, breath sounds
were heard bilaterally, with no acute cardiopulmonary issues
identified. A bruise was identified on the lower abdomen,
which was thought to be a potential seatbelt sign. A focused
assessment with sonography for trauma was negative, and an
ultrasound of additional chest and mediastinal structures was
performed for the chest tenderness.
Volume 16, Issue 7, December 2015.
Tara Murphy, et al.
Posterior reversible encephalopathy syndrome (PRES) is an unusual condition typified by acute
visual impairment caused by sudden, marked parieto-occipital vasogenic edema. Thought to be
inflammatory in origin, it has been described in patients undergoing chemotherapy, with autoimmune
disease, and in some infections. We report a case of PRES that occurred one week after an episode
of acute pancreatitis in an otherwise healthy 40-year-old female. There was progressive visual
impairment over a 24-hour period with almost complete visual loss, with characteristic findings on
magnetic resonance imaging. After treatment with steroids, the visual loss recovered. Clinicians
should retain an index of suspicion of this rare condition in patients with visual impairment after acute
pancreatitis.
Volume 16, Issue 7, December 2015.
Jesse Z. Kellar, MD, et al.
A 14-year-old African American male presented to the emergency department with worsening left
eye redness, swelling, and vision loss over the preceding three days. History was notable for similar
eye redness and swelling without vision loss four months earlier, which improved following a brief
course of prednisone. He endorsed mild eye irritation and tearing with bright lights. There was
no history of fever, respiratory symptoms or trauma. Mother was medicating patient with leftover
antibiotic eye drops x3 days without improvement. Physical examination on presentation notable
for proptosis of left eye, lid, and periorbital swelling, mild scleral injection, and central vision loss in
affected eye (20/200 OS, 20/25 OD). Extraocular movements and pupillary exam were normal. No
corneal fluorescein uptake, abnormal cell, flare, or siedel sign were seen during slit lamp exam. Eye
pressures were 24 mmHg in both eyes. Bedside ultrasonography was performed (Figure 1 showing
retinal detachment, Ultrasound Video 2 showing detachment in orbital scan).
Volume 16, Issue 7, December 2015.
Erik A. Berg, MD
A 60-year-old female with a history of
ventriculoperitoneal shunt (VPS) placement three years
prior presented with a painful abdominal wall mass.
The patient denied fevers, nausea, vomiting, headaches,
or dizziness. Physical exam revealed an afebrile, wellappearing
female with a raised, erythematous, fluctuant mass
on the right lower abdominal wall. She had no abdominal
tenderness otherwise. Labs were unremarkable. A bedside
ultrasound revealed a complex fluid collection over the
area of fluctuance that tracked along the course of the VPS
tubing into the abdomen. Plan for incision and drainage was
deferred. Neurosurgery was consulted. The neurosurgeon
attempted to tap the shunt but encountered very high
resistance. The patient was admitted for intravenous antibiotics for VPS infection and malfunction.
Volume 16, Issue 7, December 2015.
Sean P. Nordt, MD, PharmD, et al.
A 37-year-old male presented to the emergency
department (ED) in police custody for “medical clearance”
before being taken to jail. The patient was approached by
police officers for suspicion of selling illicit drugs. When
approached by police he ran away and was witnessed to
swallow several small plastic baggies suspected to contain
heroin. He was apprehended and brought to the ED.
On arrival, he was asymptomatic with a blood pressure
144/83mmHg, heart rate 67bpm, respiratory rate of 19bpm,
oxygen saturation of 99% on room air and afebrile. A Glasgow
coma score was 15 and he was alert and oriented to person,
place and time. Patient had a negative review of systems.
On physical examination pupils were 4mm and reactive to
light, lungs clear to auscultation and had normal respiratory
rate with normal cardiovascular exam. Abdomen was soft,
non-tender and non-distended with present bowel sounds.
The patient admitted to ingesting approximately 20 packets
of heroin to avoid being charged with possession. The patient
declined activated charcoal and whole bowel irrigation (WBI)
with polyethylene glycol-electrolyte solution (PEG-ELS). The
patient declined a urine toxicology immunoassay screen. A
computed tomography (CT) of his abdomen with contrast was
obtained and read as normal except for a cluster of foreign
bodies within the distal stomach likely contained within a
plastic bag.
Volume 16, Issue 7, December 2015.
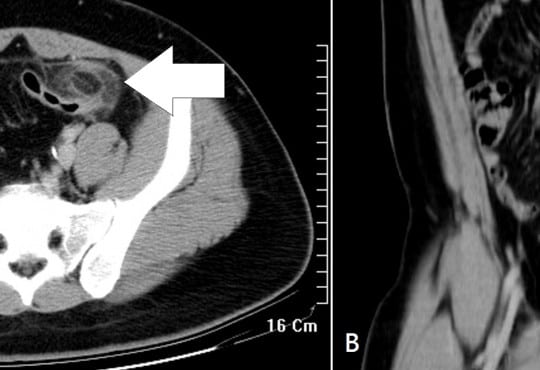
Po-Jen Yang, MD, et al.
A previously healthy 27-year-old man presented to the
emergency department with a three-day history of left lower
quadrant pain. He denied fever, nausea, vomiting, or diarrhea.
Vital signs were unremarkable, and physical examination
revealed tenderness in the left iliac fossa without peritoneal
signs. His leukocyte count and C-reactive protein were slightly
elevated. On abdominal computed tomography (CT) (Figure),
a fatty ovoid mass abutting sigmoid colon demonstrated the
infarcted or inflamed appendix epiploica. A surrounding
hyperdense rim (hyperattenuating ring sign) represented the
inflamed visceral peritoneal covering, and the central linear
hyperdensity corresponded to the thrombosed central vessel.
Volume 16, Issue 7, December 2015.
Jonathan G. Wagner, MD, et al.
A 52-year-old African American male with a long history of poorly controlled hypertension presented
to the emergency department (ED) with two days of genital edema and pain. During ED work-up,
the patient developed sudden onset of non-pitting, non-pruritic, and non-urticarial upper lip edema.
Review of his antihypertensive medication list revealed that he normally took benazepril, highly
suggestive of a diagnosis of angiotensin-converting-enzyme inhibitor-related angioedema (ACEIRA).
We present the first reported case of penile ACEI-RA that progressed to involve the oropharynx.
The ED management of the condition and some of the newer treatment options available for ACEIRA
is also briefly discussed.
Volume 16, Issue 7, December 2015.
Leonieke Groot, MD, et al.
Introduction: Currently, it is common practice in the emergency department (ED) for pain relief
in hip-fracture patients to administer pain medication, commonly systemic opioids. However, with
these pain medications come a high risk of side effects, especially in elderly patients. This study
investigated the safety profile and success rate of fascia iliaca compartment block (FICB) in a
busy ED. This ED was staffed with emergency physicians (EPs) and residents of varying levels of
experience. This study followed patients’ pain levels at various hourly intervals up to eight hours
post procedure.
Methods: Between September 2012 and July 2013, we performed a prospective pilot study on
hip-fracture patients who were admitted to the ED of a teaching hospital in the Netherlands. These
patients were followed and evaluated post FICB for pain relief. Secondary outcome was the use of
opioids as rescue medication.
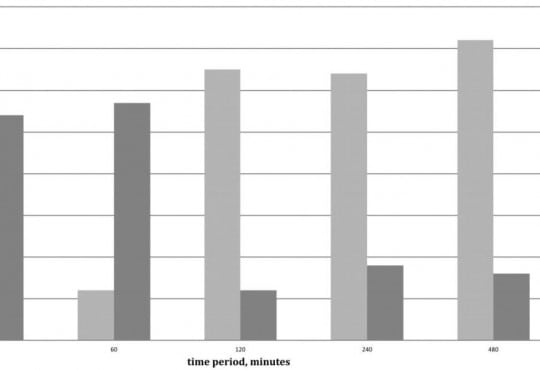
Results: Of the 43 patients in this study, patients overall experienced less pain after the FICB
(p=0.04). This reduction in pain was studied in conjunction with the use and non-use of opioids. A
clinically meaningful decrease in pain was achieved after 30 minutes in 62% of patients (54% with
the use of opioids, 8% without opioids); after 240 minutes in 82% of patients (18% with opioids, 64%
without opioids); after 480 minutes in 88% of patients (16% with opioids, 72% without opioids). No
adverse events were reported.
Conclusion: In a busy Dutch ED with rotating residents of varying levels of experience, FICB seems
to be an efficient, safe and practical method for pain reduction in patients with a hip fracture. Even
without the use of opioids, pain reduction was achieved in 64% of patients after four hours and in
72% of patients after eight hours.
Volume 16, Issue 7, December 2015.
Peter Moffett, MD, et al.
A 65-year-old male presented to the emergency department
complaining of two hours of severe lower abdominal
pain radiating into his left testicle. The patient described a
vascular procedure in the past but did not recall the details.
An emergent bedside ultrasound was performed to evaluate
the abdominal aorta. During the exam an echogenic object
consistent with a prior endovascular stent was discovered
in the distal aorta prompting further ultrasound evaluation
of the iliac artery (Figure). A true lumen (thin black arrow)
was visualized with evidence of leak (white arrows) during
color Doppler evaluation. The patient was taken emergently
to computed tomography and the diagnosis of an iliac artery
pseudoaneurysm from an endoleak was confirmed.
Volume 16, Issue 7, December 2015.
Brandon Fetterolf, DO, et al.
A 35-year-old male presented with lower gum
pain associated with fever, chills, and sore throat. His
medical history included intravenous drug use, human
immunodeficiency virus infection, and hepatitis C. Physical
exam revealed tachycardia, a temperature of 38.9°C, anterior
cervical lymphadenopathy, halitosis, an edematous lower lip,
and purulent ulcers anterior and posterior to lower central
incisors with marked tenderness and erythema (Figure).
His laboratory work was notable for a low white blood cell
count (2.6 thousand/µl), neutropenia (0.11 thousand/µl), a
low absolute CD4 lymphocyte count (0.5 thousand/µl), and
elevated C-reactive protein (129mg/L) and sedimentation
rate (23mm/hr). A computed tomography study showed a
0.5×1.3×0.3cm abscess anterior to the mandibular symphysis.
Volume 16, Issue 7, December 2015.
Sarah E. Frasure, MD, et al.
A 42-year-old female presented to the emergency
department with diffuse abdominal pain, vaginal discharge,
and a fever of 102°F. She described multiple recent male
sexual partners, with inconsistent condom use. Her vital
signs were unremarkable. Her physical exam was notable for
moderate right lower quadrant tenderness to palpation. There
was no cervical motion tenderness. The emergency physician
performed a bedside abdominal ultrasound (Video), and
subsequently ordered a computed tomography (Figure), which
confirmed the diagnosis.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 41-year-old female presented to the emergency
department with nausea, vomiting and foreign body sensation
in her throat. The patient had multiple co-morbidities including
hypertension, diabetes, cervical cancer and gastroparesis with
gastrojejunostomy (GJ) tube. The patient had stable vitals, was
in no respiratory distress, and her only complaint was mild throat
pain and abdominal pain at the GJ tube insertion site. Physical
exam revealed a foreign object in the oropharynx (Figure 1).
Abdominal exam showed a soft, non-distended, non-tender
abdomen with GJ-tube and colostomy in place. Abdominal series
and upright chest radiograph were obtained (Figure 2).
Volume 16, Issue 7, December 2015.
Marc A. Polacco, MD, et al.
Often discovered only after an extensive work up for hemoptysis and hematemesis, vallecular varices
are a rare cause of oral bleeding that increase patient morbidity due to delay of diagnosis.
We describe an 89-year-old male who presented with a week of intermittent oral blood production. A
vallecular varix was identified on fiberoptic laryngoscopy after studies for hematemesis and hemoptysis
had been performed, including negative esophagogastroduodenoscopy and bronchoscopy.
Awareness of this pathology and key points in the patient history can direct the clinician toward the
correct diagnosis, expediting treatment and limiting invasive diagnostic procedures for pulmonary or
gastric etiologies of bleeding.
Volume 16, Issue 7, December 2015.
Brian J. Wolk, MD
A 66-year-old female was transferred from an outside
hospital for possible ST segment elevation myocardial
infarction (STEMI). The patient reported feeling poorly for the
last day, with epigastric pain, nausea, and multiple episodes
of vomiting. Patient’s medical history was significant for
diabetes mellitus, hypertension, atrial fibrillation, and multiple
sclerosis. Electrocardiogram (EKG) was as noted (Figure).
Initial troponin was 0.14 (<0.03ng/mL). The patient was
taken emergently to the cardiac cath lab for possible posterior
STEMI. Angiogram demonstrated no significant evidence of
coronary artery disease, with an EF of 75%.
Volume 16, Issue 7, December 2015.
Lauren M. Porter, DO, et al.
A 42-year-old male was assisted from a car in front
of our inner city stand-alone emergency department (ED)
with a stab wound to the right chest. He was confused and
bleeding; his past medical history was unknown. The patient
was diaphoretic, pale and confused with a large vertical stab
wound over his right chest with no other obvious injuries.
On initial exam in the outlying ED, his back was obscured
by blood. He was transferred to the trauma center where
during a full secondary survey a 2cm wound was located over
the patient’s lumbar spine. The patient was stabilized and
taken for imaging. No focused assessment with sonography
for trauma (FAST) was done at either site; however, the
FAST exam, which emphasizes the search for extraluminal
blood, would not have been expected to find a foreign body
Volume 16, Issue 7, December 2015.
Krystal Garcia, BS, et al.
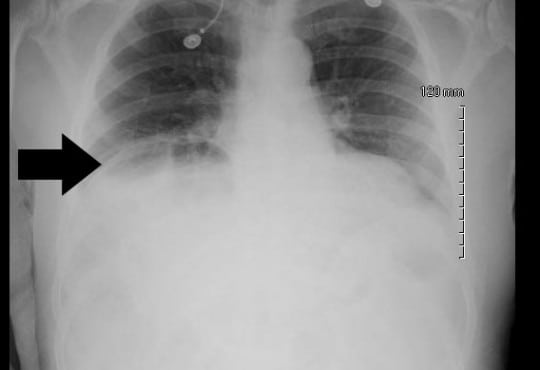
A 68-year-old male with a history of prostate cancer
presented with a two-day history of fever and left flank pain.
Vital signs included a temperature of 39.4 degrees Celsius with
93% oxygen saturation and heart rate of 112 beats per minute. An
upright chest radiograph showed concern for free intraperitoneal
air (Figure) with a white blood cell count of 17.3. A computed
tomography of the abdomen and pelvis revealed a Chilaiditi sign
with pyelonephritis, which was confirmed on urinalysis. He was
admitted for intravenous antibiotics.
Volume 16, Issue 7, December 2015.
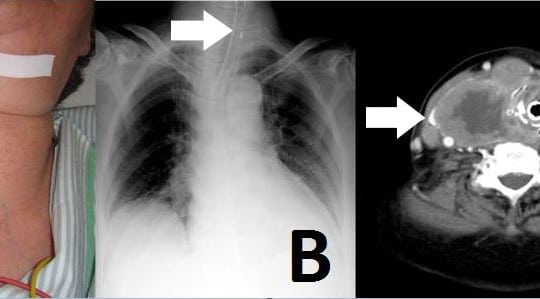
Yudai Iwasaki, MD
An 81-year-old woman was admitted to our emergency
department (ED) with neck swelling (Figure 1A) and
advancing dyspnea. Stridor was noted on auscultation of
her neck, and her breathing was labored. We immediately
diagnosed airway obstruction, and emergency intubation was
performed using a video laryngoscope (AWS-S100L®, Pentax
Corporation, Tokyo, Japan). The epiglottis was found to have
shifted to the left on chest video images and chest radiograph.
Volume 16, Issue 5, September 2015.
Thomas M. Nappe, Do, et al.
A 56-year-old female presented to the emergency
department (ED) with a chief complaint of urinary retention
and overflow incontinence for 24 hours, preceded by
progressive difficulty with voiding, worsening lower
abdominal discomfort and bloating. Her past medical
history was significant for small bowel obstruction and
neurofibromatosis with an associated benign pelvic tumor that
caused similar symptoms as a child, but had been known to
be stable since that time. She had also recently been treated
for a urinary tract infection. Her physical exam revealed
tachycardia and a diffusely tender abdomen with a palpable,
tender suprapubic mass extending just above her umbilicus.
Volume 16, Issue 5, September 2015.
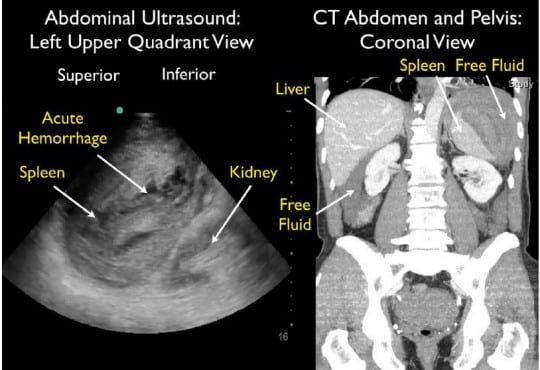
William Mulkerin, MD, et al.
A 64-year-old male presented to the emergency
department (ED) with near syncope and worsening left flank
and shoulder pain. He had undergone a difficult colonoscopy
two days prior due to a tortuous colon. Initial vital signs
were normal. He looked uncomfortable and had significant
left upper quadrant abdominal tenderness with guarding.
Thirty minutes after ED arrival, his blood pressure dropped
to 73/59 mmHg, requiring aggressive fluid resuscitation.
Bedside focused assessment with sonography in trauma
(FAST) exam demonstrated free fluid in the abdomen with
mixed echogenicity of the spleen, suggestive of splenic injury.
Computed tomography (CT) demonstrated a large subcapsular
splenic hematoma with active extravasation and surrounding
intraperitoneal free fluid.
{kind=link}