Volume 16, Issue 7, December 2015.
Sean P. Nordt, MD, PharmD, et al.
A 37-year-old male presented to the emergency
department (ED) in police custody for “medical clearance”
before being taken to jail. The patient was approached by
police officers for suspicion of selling illicit drugs. When
approached by police he ran away and was witnessed to
swallow several small plastic baggies suspected to contain
heroin. He was apprehended and brought to the ED.
On arrival, he was asymptomatic with a blood pressure
144/83mmHg, heart rate 67bpm, respiratory rate of 19bpm,
oxygen saturation of 99% on room air and afebrile. A Glasgow
coma score was 15 and he was alert and oriented to person,
place and time. Patient had a negative review of systems.
On physical examination pupils were 4mm and reactive to
light, lungs clear to auscultation and had normal respiratory
rate with normal cardiovascular exam. Abdomen was soft,
non-tender and non-distended with present bowel sounds.
The patient admitted to ingesting approximately 20 packets
of heroin to avoid being charged with possession. The patient
declined activated charcoal and whole bowel irrigation (WBI)
with polyethylene glycol-electrolyte solution (PEG-ELS). The
patient declined a urine toxicology immunoassay screen. A
computed tomography (CT) of his abdomen with contrast was
obtained and read as normal except for a cluster of foreign
bodies within the distal stomach likely contained within a
plastic bag.
Volume 16, Issue 7, December 2015.
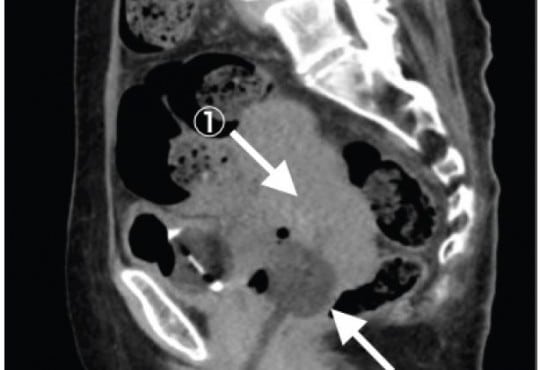
Po-Jen Yang, MD, et al.
A previously healthy 27-year-old man presented to the
emergency department with a three-day history of left lower
quadrant pain. He denied fever, nausea, vomiting, or diarrhea.
Vital signs were unremarkable, and physical examination
revealed tenderness in the left iliac fossa without peritoneal
signs. His leukocyte count and C-reactive protein were slightly
elevated. On abdominal computed tomography (CT) (Figure),
a fatty ovoid mass abutting sigmoid colon demonstrated the
infarcted or inflamed appendix epiploica. A surrounding
hyperdense rim (hyperattenuating ring sign) represented the
inflamed visceral peritoneal covering, and the central linear
hyperdensity corresponded to the thrombosed central vessel.
Volume 16, Issue 7, December 2015.
Jonathan G. Wagner, MD, et al.
A 52-year-old African American male with a long history of poorly controlled hypertension presented
to the emergency department (ED) with two days of genital edema and pain. During ED work-up,
the patient developed sudden onset of non-pitting, non-pruritic, and non-urticarial upper lip edema.
Review of his antihypertensive medication list revealed that he normally took benazepril, highly
suggestive of a diagnosis of angiotensin-converting-enzyme inhibitor-related angioedema (ACEIRA).
We present the first reported case of penile ACEI-RA that progressed to involve the oropharynx.
The ED management of the condition and some of the newer treatment options available for ACEIRA
is also briefly discussed.
Volume 16, Issue 7, December 2015.
Leonieke Groot, MD, et al.
Introduction: Currently, it is common practice in the emergency department (ED) for pain relief
in hip-fracture patients to administer pain medication, commonly systemic opioids. However, with
these pain medications come a high risk of side effects, especially in elderly patients. This study
investigated the safety profile and success rate of fascia iliaca compartment block (FICB) in a
busy ED. This ED was staffed with emergency physicians (EPs) and residents of varying levels of
experience. This study followed patients’ pain levels at various hourly intervals up to eight hours
post procedure.
Methods: Between September 2012 and July 2013, we performed a prospective pilot study on
hip-fracture patients who were admitted to the ED of a teaching hospital in the Netherlands. These
patients were followed and evaluated post FICB for pain relief. Secondary outcome was the use of
opioids as rescue medication.
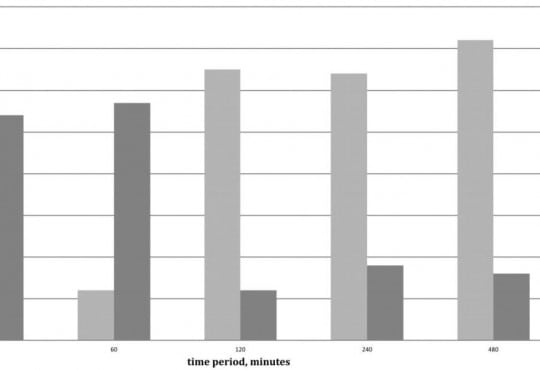
Results: Of the 43 patients in this study, patients overall experienced less pain after the FICB
(p=0.04). This reduction in pain was studied in conjunction with the use and non-use of opioids. A
clinically meaningful decrease in pain was achieved after 30 minutes in 62% of patients (54% with
the use of opioids, 8% without opioids); after 240 minutes in 82% of patients (18% with opioids, 64%
without opioids); after 480 minutes in 88% of patients (16% with opioids, 72% without opioids). No
adverse events were reported.
Conclusion: In a busy Dutch ED with rotating residents of varying levels of experience, FICB seems
to be an efficient, safe and practical method for pain reduction in patients with a hip fracture. Even
without the use of opioids, pain reduction was achieved in 64% of patients after four hours and in
72% of patients after eight hours.
Volume 16, Issue 7, December 2015.
Peter Moffett, MD, et al.
A 65-year-old male presented to the emergency department
complaining of two hours of severe lower abdominal
pain radiating into his left testicle. The patient described a
vascular procedure in the past but did not recall the details.
An emergent bedside ultrasound was performed to evaluate
the abdominal aorta. During the exam an echogenic object
consistent with a prior endovascular stent was discovered
in the distal aorta prompting further ultrasound evaluation
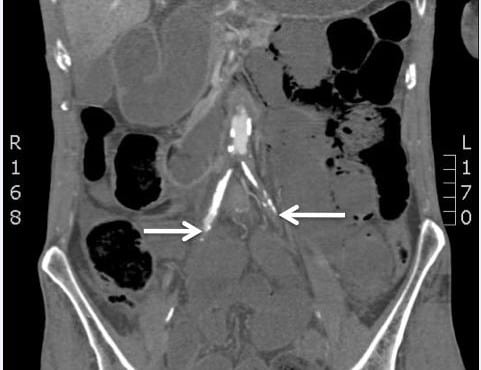
of the iliac artery (Figure). A true lumen (thin black arrow)
was visualized with evidence of leak (white arrows) during
color Doppler evaluation. The patient was taken emergently
to computed tomography and the diagnosis of an iliac artery
pseudoaneurysm from an endoleak was confirmed.
Volume 16, Issue 7, December 2015.
Brandon Fetterolf, DO, et al.
A 35-year-old male presented with lower gum
pain associated with fever, chills, and sore throat. His
medical history included intravenous drug use, human
immunodeficiency virus infection, and hepatitis C. Physical
exam revealed tachycardia, a temperature of 38.9°C, anterior
cervical lymphadenopathy, halitosis, an edematous lower lip,
and purulent ulcers anterior and posterior to lower central
incisors with marked tenderness and erythema (Figure).
His laboratory work was notable for a low white blood cell
count (2.6 thousand/µl), neutropenia (0.11 thousand/µl), a
low absolute CD4 lymphocyte count (0.5 thousand/µl), and
elevated C-reactive protein (129mg/L) and sedimentation
rate (23mm/hr). A computed tomography study showed a
0.5×1.3×0.3cm abscess anterior to the mandibular symphysis.
Volume 16, Issue 7, December 2015.
Sarah E. Frasure, MD, et al.
A 42-year-old female presented to the emergency
department with diffuse abdominal pain, vaginal discharge,
and a fever of 102°F. She described multiple recent male
sexual partners, with inconsistent condom use. Her vital
signs were unremarkable. Her physical exam was notable for
moderate right lower quadrant tenderness to palpation. There
was no cervical motion tenderness. The emergency physician
performed a bedside abdominal ultrasound (Video), and
subsequently ordered a computed tomography (Figure), which
confirmed the diagnosis.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 41-year-old female presented to the emergency
department with nausea, vomiting and foreign body sensation
in her throat. The patient had multiple co-morbidities including
hypertension, diabetes, cervical cancer and gastroparesis with
gastrojejunostomy (GJ) tube. The patient had stable vitals, was
in no respiratory distress, and her only complaint was mild throat
pain and abdominal pain at the GJ tube insertion site. Physical
exam revealed a foreign object in the oropharynx (Figure 1).
Abdominal exam showed a soft, non-distended, non-tender
abdomen with GJ-tube and colostomy in place. Abdominal series
and upright chest radiograph were obtained (Figure 2).
Volume 16, Issue 7, December 2015.
Marc A. Polacco, MD, et al.
Often discovered only after an extensive work up for hemoptysis and hematemesis, vallecular varices
are a rare cause of oral bleeding that increase patient morbidity due to delay of diagnosis.
We describe an 89-year-old male who presented with a week of intermittent oral blood production. A
vallecular varix was identified on fiberoptic laryngoscopy after studies for hematemesis and hemoptysis
had been performed, including negative esophagogastroduodenoscopy and bronchoscopy.
Awareness of this pathology and key points in the patient history can direct the clinician toward the
correct diagnosis, expediting treatment and limiting invasive diagnostic procedures for pulmonary or
gastric etiologies of bleeding.
Volume 16, Issue 7, December 2015.
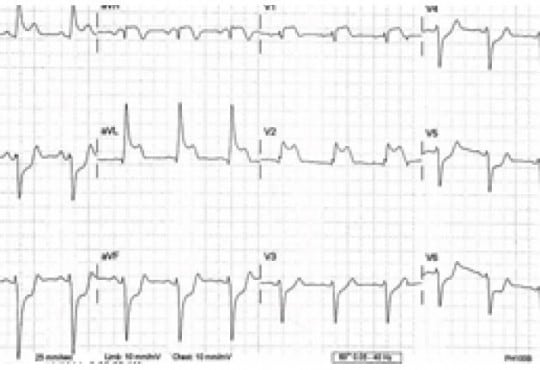
Brian J. Wolk, MD
A 66-year-old female was transferred from an outside
hospital for possible ST segment elevation myocardial
infarction (STEMI). The patient reported feeling poorly for the
last day, with epigastric pain, nausea, and multiple episodes
of vomiting. Patient’s medical history was significant for
diabetes mellitus, hypertension, atrial fibrillation, and multiple
sclerosis. Electrocardiogram (EKG) was as noted (Figure).
Initial troponin was 0.14 (<0.03ng/mL). The patient was
taken emergently to the cardiac cath lab for possible posterior
STEMI. Angiogram demonstrated no significant evidence of
coronary artery disease, with an EF of 75%.
Volume 16, Issue 7, December 2015.
Lauren M. Porter, DO, et al.
A 42-year-old male was assisted from a car in front
of our inner city stand-alone emergency department (ED)
with a stab wound to the right chest. He was confused and
bleeding; his past medical history was unknown. The patient
was diaphoretic, pale and confused with a large vertical stab
wound over his right chest with no other obvious injuries.
On initial exam in the outlying ED, his back was obscured
by blood. He was transferred to the trauma center where
during a full secondary survey a 2cm wound was located over
the patient’s lumbar spine. The patient was stabilized and
taken for imaging. No focused assessment with sonography
for trauma (FAST) was done at either site; however, the
FAST exam, which emphasizes the search for extraluminal
blood, would not have been expected to find a foreign body
Volume 16, Issue 7, December 2015.
Krystal Garcia, BS, et al.
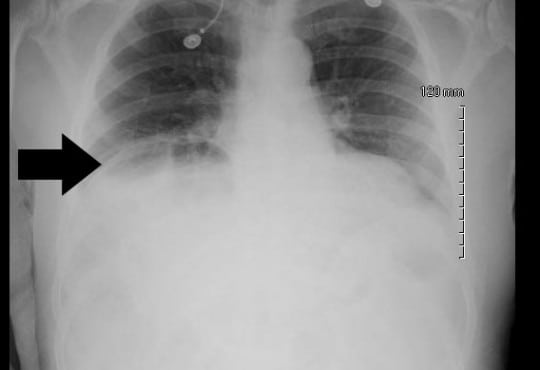
A 68-year-old male with a history of prostate cancer
presented with a two-day history of fever and left flank pain.
Vital signs included a temperature of 39.4 degrees Celsius with
93% oxygen saturation and heart rate of 112 beats per minute. An
upright chest radiograph showed concern for free intraperitoneal
air (Figure) with a white blood cell count of 17.3. A computed
tomography of the abdomen and pelvis revealed a Chilaiditi sign
with pyelonephritis, which was confirmed on urinalysis. He was
admitted for intravenous antibiotics.
Volume 16, Issue 7, December 2015.
Yudai Iwasaki, MD
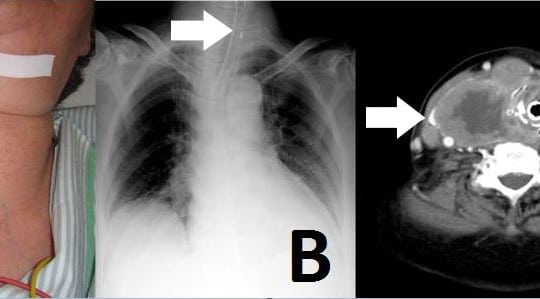
An 81-year-old woman was admitted to our emergency
department (ED) with neck swelling (Figure 1A) and
advancing dyspnea. Stridor was noted on auscultation of
her neck, and her breathing was labored. We immediately
diagnosed airway obstruction, and emergency intubation was
performed using a video laryngoscope (AWS-S100L®, Pentax
Corporation, Tokyo, Japan). The epiglottis was found to have
shifted to the left on chest video images and chest radiograph.
Volume 16, Issue 5, September 2015.
Caroline T. Brandon, MD, et al.
A 34-year-old male with diabetes presented to the
emergency department with four days of progressively
worsening redness, swelling and pain to his left buttock.
The patient denied fevers, chills, rectal pain or purulent
drainage from his rectum. His initial vital signs were heart
rate of 82; blood pressure of 146/92; and temperature of
98.2°F. The left buttock had a poorly circumscribed area of
induration; however, there was no fluctuance or crepitace.
Rectal exam was unremarkable. Because the patient’s
buttock pain was disproportionate to his exam findings,
a point-of-care ultrasound was performed to determine
if a more extensive process was present. The ultrasound
demonstrated cobblestoning, fascial thickening with edema,
and a large 4.5cm fluid collection extending and adjacent
to the rectum.
Volume 16, Issue 5, September 2015.
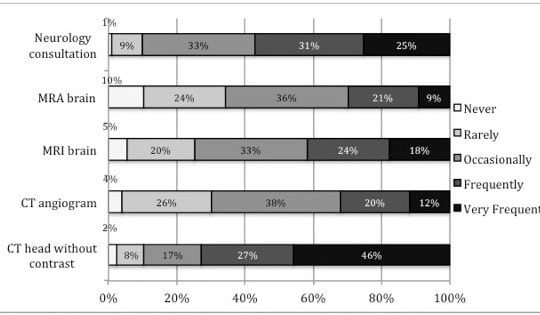
Mamata V. Kene, MD, MPH, et al.
Introduction: We evaluated emergency physicians’ (EP) current perceptions, practice, and attitudes
towards evaluating stroke as a cause of dizziness among emergency department patients.
Methods: We administered a survey to all EPs in a large integrated healthcare delivery system.
The survey included clinical vignettes, perceived utility of historical and exam elements, attitudes
about the value of and requisite post-test probability of a clinical prediction rule for dizziness. We
calculated descriptive statistics and post-test probabilities for such a clinical prediction rule.
Results: The response rate was 68% (366/535). Respondents’ median practice tenure was
eight years (37% female, 92% emergency medicine board certified). Symptom quality and typical
vascular risk factors increased suspicion for stroke as a cause of dizziness. Most respondents
reported obtaining head computed tomography (CT) (74%). Nearly all respondents used and
felt confident using cranial nerve and limb strength testing. A substantial minority of EPs used
the Epley maneuver (49%) and HINTS (head-thrust test, gaze-evoked nystagmus, and skew
deviation) testing (30%); however, few EPs reported confidence in these tests’ bedside application
(35% and 16%, respectively). Respondents favorably viewed applying a properly validated clinical
prediction rule for assessment of immediate and 30-day stroke risk, but indicated it would have to
reduce stroke risk to <0.5% to be clinically useful.
Conclusion: EPs report relying on symptom quality, vascular risk factors, simple physical exam
elements, and head CT to diagnose stroke as the cause of dizziness, but would find a validated
clinical prediction rule for dizziness helpful. A clinical prediction rule would have to achieve a 0.5%
post-test stroke probability for acceptability.
Volume 16, Issue 5, September 2015.
Daniel Miller, MD
Emergency physicians are often required to evaluate and treat undifferentiated patients suffering
acute hemodynamic compromise (AHC). It is helpful to apply a structured approach based on a
differential diagnosis including all causes of AHC that can be identified and treated during a primary
assessment. Tension pneumoperitoneum (TP) is an uncommon condition with the potential to be
rapidly fatal. It is amenable to prompt diagnosis and stabilization in the emergency department. We
present a case of a 16-year-old boy with TP to demonstrate how TP should be incorporated into a
differential diagnosis when evaluating an undifferentiated patient with AHC.
Volume 16, Issue 5, September 2015
Christian Jensen, DO, et al.
Sumitriptan has been used by millions as a migraine abortant; however, there have been studies
showing angina pectoris, coronary vasospasm, and even myocardial infarction in patients with
predisposing cardiac risk factors. The majority are patients using the injectable form subcutaneously.
We present the case of a patient who presents with ST-elevation myocardial infarction, with no
cardiovascular risk factors, after ingesting oral sumitriptan for her typical migraine.
Volume 16, Issue 5, September 2015
Jill Tirabassi, MD, et al.
A 25-year-old male presented to the ski clinic after
colliding with a tree while snowboarding. He had immediate
sharp pain at his “tailbone,” but denied numbness and
weakness. Past medical history was initially reported as
unremarkable. On exam, he demonstrated midline tenderness
over the sacrum. Pelvic radiography was performed (Figure).
Volume 16, Issue 5, September 2015
Jagdipak Heer, MD, et al.
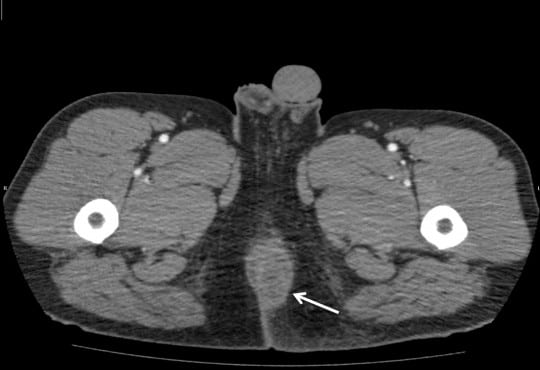
A 31-year-old gravida 3 Para 3 female with no past
medical history, presented to the emergency department
complaining of a painless “boil” to the right groin, which
had been enlarging for over two months. Although it
was generally painless, she did suffer mild dyspareunia
at times. Antibiotics prescribed by her primary doctor
failed to resolve this mass so she decided to present to the
emergency department.
Volume 16, Issue 5, September 2015.
Stephen L. Thornton, MD, et al.
A previously healthy two-year-old boy presented to the
emergency department with vomiting. He was cyanotic with
mottling of both lower extremities. He was in respiratory
distress with retractions and diminished breath sounds. His
abdomen was distended and rigid. He had a pulse of 170 beats
per minute, blood pressure of 144/69mmHg and respiratory
rate of 42 breaths per minute. He was endotracheally
intubated. Chest and abdominal radiographs demonstrated a
tension pneumoperitoneum.
Volume 16, Issue 5, September 2015.
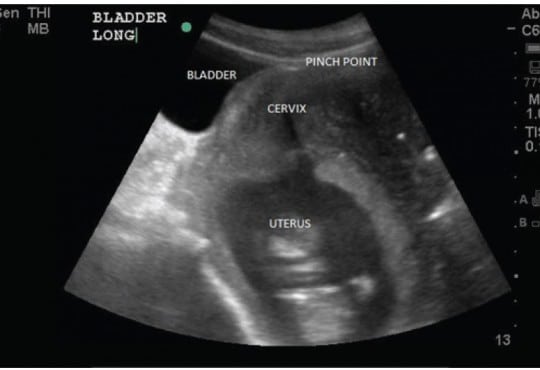
Richard Slama, MD, et al.
Gravid uterine incarceration (GUI) is a condition that is well discussed in literature; however, there
are few acute diagnoses in the emergency department (ED). We present a case series where
three multiparous females presented to the ED with non-specific urinary symptoms. On bedside
ultrasound, each patient was noted to have a retroverted uterus and inferior bladder entrapment
under the sacral promontory. GUI is a rare condition that can lead to uremia, sepsis, peritonitis, and
ultimately maternal death. Emergency physicians should include GUI in their differential diagnosis in
this patient population and use bedside ultrasound as an adjunct to diagnosis.
Volume 16, Issue 5, September 2015.
Tomohiro Sonoo, MD, et al.
A 67-year-old woman complaining of continuous fresh
vaginal hemorrhage came to our emergency department in a
pre-shock state. Examinations revealed an irregularly shaped
mass in the uterus and active arterial bleeding. Emergent
hysterectomy and interventional radiology were not
immediately available. Foley catheter with 20mL water was
inserted into the uterine cavity, then the balloon was pulled
to obstruct the uterus output (Figure). Her vital signs became
stabilized, and she was transferred to another hospital two
days later.
Volume 16, Issue 4, July 2015.
Patrick Burns, MD, et al.
A 48-year-old male presented with body aches and a chronic rash. He had no medical history aside from two unsuccessful treatments for presumed scabies and a recent diagnosis of psoriasis. Physical exam revealed hypotension, tachycardia, and profound, diffuse yellow crusting of the skin with erythematous erosions covering non-crusted areas. The patient was resuscitated and treated for septic shock while microscopic evaluation of scrapings of the crusted skin was performed.
Volume 16, Issue 4, July 2015.
C. Eric McCoy, MD, MPH, et al.
Leriche syndrome, also referred to as aortoiliac
occlusive disease, has been described as a triad of
claudication, impotence and decreased femoral pulses.
The syndrome results from thrombotic aortoiliac occlusion and
was first described by a French surgeon, Rene Leriche, in
1940. The disease most commonly occurs in men, and risk
factors include hypertension, diabetes, hyperlipidemia, and
smoking.
Volume 16, Issue 4, July 2015.
Nobuhiko Kimura, MD, et al.
A 30-year-old man presented to the emergency department
for two weeks of diffuse abdominal pain and an episode of
emesis. He denied fever, prior surgery, or any other illnesses.
The patient reported going on a “crash diet regimen” one
month prior, resulting in an intentional weight loss of 25lbs in
30 days.
A 26-year-old female presented to the emergency department with a chief complaint of dizziness. Further history revealed that she was experiencing generalized weakness and intractable vomiting for three days, without complaint of abdominal pain or lower gastrointestinal symptoms. Physical examination uncovered mild dehydration with stable vital signs and non-fatigable, horizontal nystagmus consistent with internuclear opthalmoplegia.
{kind=link}