
{kind=link}
| Author | Affiliation |
|---|---|
| Kirk A. Stiffler, MD | Summa Health System/Northeastern Ohio Universities College of Medicine |
| Scott T. Wilber, MD, MPH | Summa Health System/Northeastern Ohio Universities College of Medicine |
ABSTRACT
Introduction:
Our objective was to assess the reported driving patterns of older emergency department (ED) drivers and the factors that might lead them to enroll in a safe driving program.
Methods:
We conducted a prospective, cross-sectional survey of a convenience sample of ED patients 65-years-old and up regarding their driving patterns, behaviors and willingness to enroll in a safe driving program.
Results:
We surveyed 138 patients. Most (73%) reported driving within the last year, and 88% of these believe they could not manage without driving. Eleven percent of ED older drivers have been in a motor vehicle crash (MVC) in the past year (95% CI 6–20%), compared to 2.5% of all seniors. Our survey findings suggest that 88% of older ED drivers avoid at least some high-risk driving situations and 65% are unwilling to enroll in a safe driver program unless it lowers their automobile insurance rates. At the same time, most older ED drivers underestimate their risk of being involved in (75%) or dying from (74%) a MVC.
Conclusion:
Overall, there are a significant number of older people for whom driving remains a vital yet risky daily function. Most of these drivers have little interest in information regarding safe driving programs while in the ED. Those willing to learn about such programs would prefer to take home the information regarding the program rather than have any staff member discuss it while in the ED.
INTRODUCTION
The proportion of persons 65-years-old and over is increasing dramatically.1 Automobile licensing rates will likely increase among the elderly.2 Even without this impending demographic surge, there were already 30 million licensed older drivers in the U.S. in 2006. This represents an 18% increase from 1996, while the total number of licensed drivers increased by only 13% during the same time period.3 Ninety percent of adults in the United States over age 65 rely upon private automobiles for transportation.4 This declines to 75% of community-dwelling adults over age 75 who are thus at risk of becoming transportation disadvantaged.5
Older adult driving safety is a major public health issue. More stringent licensure requirements have not reduced fatalities.6 Seventeen states have legislation requiring unique testing for older drivers.7The American Medical Association, the American Association of Retired Persons, and the National Highway Traffic Safety Administration have contributed programs, publications and guidelines to increase the safety and public awareness of older driving issues.8,9,10
Older drivers are at a higher risk of harming themselves and others compared to almost all other age groups of drivers even though they drive fewer annual miles.11,12 Factors contributing to this risk include age-related declines in vision, such as reduced acuity, light sensitivity, peripheral vision capabilities, increased glare susceptibility, and slower ocular movements.13,14 Cognitive skills allowing for rapid sequence tasking during driving compare unfavorably to younger drivers.15 Also, short and long-term memory decline with age. Determinants of functional impairment such as reaction time, strength, and coordination diminish with age.16 Prescription medications, such as benzodiazepines, antihistamines, antidepressants, analgesics and hypoglycemics, also contribute to increased crash risks.17 Many of these factors impact older drivers despite self-compensatory measures, such as cessation of nighttime and congested driving, driving fewer miles, avoiding passengers, and driving with a “co-pilot.”18–20
Emergency physicians (EP) frequently evaluate many conditions that adversely affect the perceptual, cognitive and physical motor skills required for safe driving.16,21,22 Emergency department (ED) visits may represent opportune moments for injury prevention education.23 We undertook this study to gain a better understanding of older ED patients’ driving patterns and problems and to explore their willingness to enroll in a safe driver program.24
METHODS
Study Design and Setting
We conducted a pilot, prospective, cross-sectional study in an urban, adult community teaching hospital ED (annual census 71,000). Approximately 23% of patients evaluated are aged 65 and older, and on average 35 older patients are seen in the ED daily between 7 AM and 11 PM. The hospital’s Institutional Review Board approved this study.
Study Population
We included adult ED patients 65 and older who verbally consented to answer the survey. Research technicians were available to screen patients on weekdays from 7 AM until 11 PM. However, the sampling was not consecutive, as the technicians were involved in other concurrent research studies. We excluded patients in the ED for a motor vehicle crash (MVC), admitted from a nursing home, unable to communicate in English, who never drove before, and who were too ill to participate (e.g. altered level of consciousness, severe respiratory distress, myocardial infarctions, cerebrovascular accidents, intense active nausea and vomiting)
Study Protocol
We adapted the survey from other existing surveys and studies.25,26 These questionnaires are believed to have face validity but have not been shown to have predictive ability for future MVCs.26We pre-tested our survey on five older ED patients for clarity, readability, and timing. Two research technicians administered the study. The survey queried older patients regarding their current driving patterns, perceived driving problems, and their willingness to enroll in a theoretical safe driver program. We recorded their preferences for a safe-driving program in terms of how they would prefer to obtain information, what information they would like to learn, and where they would like to attend a program.
Measurements and Data Analysis
We evaluated data with STATA®, version 8 (College Station, TX) and presented it as means and proportions with 95% confidence intervals. A confidence interval of +/– 10% for a single proportion could be obtained by enrolling 96 drivers.
RESULTS
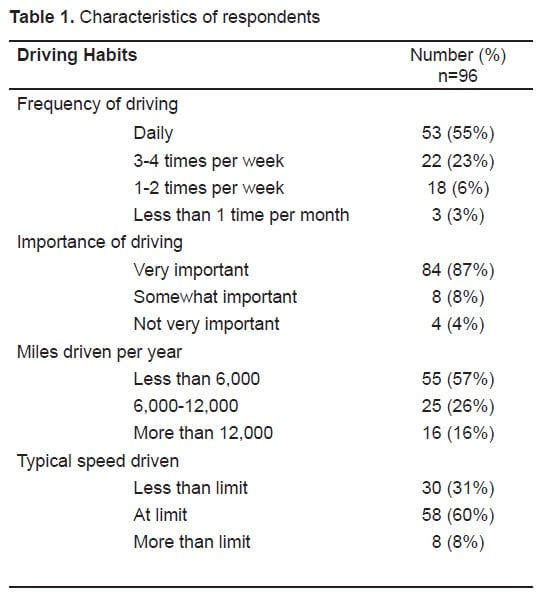
From September 2005 through January 2006, we approached 472 older ED patients. We excluded 241 patients, 50 were missed, and 43 refused. Reasons for exclusion included: too ill to participate (166), from a skilled nursing facility (48), in an MVC (5), non-English speaking (2), never drove before (19), and already enrolled (1). One hundred thirty-eight people agreed to participate. The mean age of those participating was 76 ± 6.4 standard deviation years and 51% were female. Out of these 138,101 reported having driven within the last one year (73%, 95%CI 65 – 80%), while 96 considered themselves current drivers (96/138 70% 95 CI 62–77%). Daily drivers made up 55% of current drivers (53/96 55% 95 CI 45–65%), 88% of current drivers stated they could not get along without driving (84/96 95% CI 79–94%), and 57% (55/96 95% CI 47–67%) drive somewhere between one and 6,000 miles per year (Table). Of the current drivers, 11% were involved in a crash within the past year (11/96 11% 95 CI 6–20%).
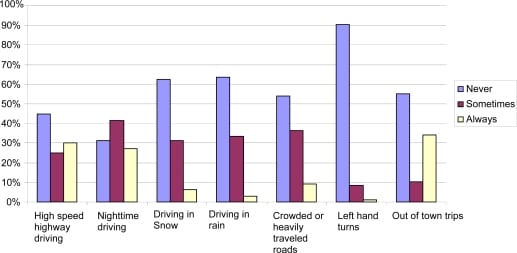
Most older drivers rated their own health compared to their peers (regardless of driving status) as either good or excellent (63/96 66% 96 CI 55–75%), while 89% (85/95 CI 81–95%) rated their driving compared to their peers as good or excellent. Three-fourths of those surveyed believe that compared to other groups, they are at the same or lower risk of both being involved in a MVC (71/95, 75%, 95% CI 65–83%) and dying in a MVC (70/94, 74%, 95% CI 64–83%) per mile driven. Older drivers reported sometimes avoiding high-risk driving behaviors, such as driving at nighttime, on highways, in inclement weather, on heavily congested routes, and for long distances (Figure).
Of the 96 current drivers, 35 (36% 95 CI 27–47%) said that they would be willing to enroll in a safe driver program. However, 79% (76/96, 95% CI 70–87%) would be more interested in enrolling if it lowered their automobile insurance rates. Older drivers preferred taking home a video (53/96, 55%, 95% CI 45–65%) or a pamphlet (31/96, 32%, 95% CI 23–43%) to having their doctor (9/96, 9.3%, 95% CI 4.3–17%), nurse (0/96, 0%, 95% CI 0–3.8%), or a senior volunteer (3/96, 3.1%, 95% CI 0.6–8.9%) discuss driving safety with them while in the ED. The content older drivers most preferred for inclusion in safe driver programs included information on how to improve overall driving abilities (67/96 70% 95 CI 60–79%), information on how aging affects driving abilities (66/96 69%, 95 CI 58–78%), and how to lower their crash risk (54/96 56% 95 CI 46–66%). Less desirable topics included on-road lessons by driving instructors (32/96, 33% 95 CI 24–44%) and information on bad weather driving (35/96, 36% 95 CI 27–47%). Most subjects would prefer to attend a safe driving program at a local church or community center (55%, 53/96, 95% CI 45–65%), as opposed to a hospital facility (42%, 41/96, 95%CI 33–53%). The remaining participants would prefer a local driving school.
DISCUSSION
Many driving programs for older drivers already exist, yet no consistent improvement in lowering crash rates has been shown.27–29 Prior to this study, the characteristics, behaviors and expectations of older drivers have not been established. Despite the fact that older drivers represent a high-risk age group for driving, the majority of older drivers do not express an understanding of this higher risk. Many of the ED drivers are frequent drivers, and it is considered very important to them. Our results concur with other surveys suggesting that older people do continue to drive using shorter trips, fewer miles, and self-imposed limitations to minimize risk, and they often describe visual and functional status limitations.30
In addition, older drivers who are in the ED for reasons unrelated to MVCs may represent a particularly high-risk group since they are involved in MVCs at a much higher rate (11% in the current study) than the general older population rate of 2.5%.31 This may be evidence that an ED visit is a marker for increased frailty and functional dependence.
Despite the potential advantages, controversy remains surrounding the screening of older drivers and upon whom the burden of proof falls to demonstrate driving abilities.32,33 Several resources are available for assessing older drivers.8,34–36 These publications cover many issues pertinent to older drivers, including physical constraints, medical problems, cognitive status and dementia, medications, and the myriad of psychosocial aspects regarding driving cessation.
EPs face unique patient care challenges. Additional cognitive, physical, medica, and social screening may be impractical for a single ED visit. Even in primary care settings, barriers to effective screening include the potential liability for screening results, the lack of uniformity and predictive ability of existing screening methods, the possibility of patients reacting unfavorably to driving assessments, and a lack of resources.37 Nonetheless, EPs must remain vigilant about the disposition of older ED drivers because nine states currently have relevant physician reporting laws.7
Overall, older drivers expressed little interest in attending a safe driver program except if it were to lower their automobile insurance rates. We were surprised that older drivers had such little interest in discussing safe driving issues with anyone while in the ED, including a senior volunteer. They did have a much greater willingness to learn via take-home materials. These issues should be taken into account when designing programs for intervention in this group. The fact that such a large percentage of the older drivers stated that they could not get along without driving may be due to the limited alternative means of transportation (such as carpooling, ridesharing, or public transit) within our community.
LIMITATIONS
There were no safe driver programs or materials offered to the study participants, therefore the impact of these on older drivers cannot be assessed. The survey has not been validated, nor been proven reliable. The nighttime exclusion, single site sampling of patients and the lack of a standard amount of alternative means of transportation may limit generalizability. In addition, neither the individual’s functional status nor the familial influences on driving decisions were assessed. Lastly, typical times and reasons for driving, existing co-morbidities, and current medication use were not assessed.
CONCLUSION
Driving appears to be a very important aspect of daily living for many older ED patients. Most underestimate the increased risk of injury or death they incur from such activity compared to the remaining population. Several high-risk driving situations are often avoided by older drivers in an attempt to minimize difficulties. ED older drivers may represent a high-risk subgroup of older drivers. However, most still demonstrate little interest in a safe driving program, if approached while in an ED, unless it were to lower their automobile insurance rates.
Footnotes
Supervising Section Editor: Teresita M Hogan, MD
Submission history: Submitted: October 21, 2009; Revision received February 18, 2010; Accepted June 15, 2010.
Reprints available through open access at http://escholarship.org/uc/uciem_westjem.
Address for Correspondence: Kirk A. Stiffler, MD, Summa Health System, Emergency Medicine Research Center, Akron City Hospital, 41 Arch St., Suite 519, Akron, Ohio 44309. Email: stifflek@summa-health.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Organization For Economic Co-operation and Development (OECD); Paris, France: 2001. Ageing and Transport: Mobility Needs and Safety Issues.
2. Eberhard J. Safe mobility for senior citizens. Journal of the International Association of Traffic and Safety Sciences. 1996;20:29–37.
3. National Highway Traffic Safety Administration, Department of Transportation (US) Washington (DC): NHTSA; 2006. Traffic Safety Facts 2006: Older Population. Available at: http://www-nrd.nhtsa.dot.gov/Pubs/810808.PDF. Accessed September 1, 2009.
4. Hu PS, Young JR. Washington, DC: U.S. DOT, Federal Highway Administration; 1999. Summary of Travel Trends 1995 National Personal Transportation Survey.
5. Flaherty JH, Stalvey B, Rubenstein L. A consensus statement on nonemergent medical transportation services for older persons. J Gerontol A Biol Sci Med Sci. 2003;58(9):M826–31.[PubMed]
6. Grabowski DC, Campbell CM, Morrisey MA. Elderly licensure laws and motor vehicle fatalities.JAMA. 2004;291(23):2840–6. [PubMed]
7. Older Driver Available at: http://www.iii.org/media/hottopics/insurance/olderdrivers/. Accessed February 8, 2010.
8. AMA Physicians Guide to Assessing and Counseling Older Drivers Available at: http://www.ama-assn.org/ama/pub/physician-resources/public-health/promoting-healthy-lifestyles/geriatric-health/older-driver-safety/assessing-counseling-older-drivers.shtml. Accessed September 14, 2009.
9. AARP Driver Safety Program Information available at:http://www.aarp.org/family/housing/driver_safety_program/driver_safety_program/
10. NHTSA Publication Driving Safely while Aging Gracefully. Available at:http://www.nhtsa.dot.gov/people/injury/olddrive/Driving%20Safely%20Aging%20Web/page8.html.
11. Li G, Braver ER, Chen LH. Fragility versus excessive crash involvement as determinants of high death rates per vehicle-mile of travel among older drivers. Accid Anal Prev. 2003;35(2):227–35.[PubMed]
12. Braver ER, Trempel RE. Are older drivers actually at higher risk of involvement in collisions resulting in deaths or non-fatal injuries among their passengers and other road users. Inj Prev.2004;10(1):27–32. [PMC free article] [PubMed]
13. Ball K, Owsley C, Stalvey B, et al. Driving avoidance and functional impairment in older drivers.Accid Anal Prev. 1998;30(3):313–22. [PubMed]
14. Owsley C, Ball K, Sloane ME, et al. Visual/cognitive correlates of vehicle accidents in older drivers. Psychol Aging. 1991;6(3):403–15. [PubMed]
15. Parker D, McDonald L, Rabbitt P, et al. Older drivers and road safety: the acceptability of a range of intervention measures. Accid Anal Prev. 2003;35(5):805–10. [PubMed]
16. Lyman JM, McGwin G, Jr, Sims RV. Factors related to driving difficulty and habits in older drivers. Accid Anal Prev. 2001;33(3):413–21. [PubMed]
17. Eby DWT, Molnar DA, Shope LJ, et al. The assessment of Older Drivers capabilities: A review of the literature. The University of Michigan, Transportation Research Institute; 1998.
18. Charlton JL, Oxley J, Fildes B, et al. Self-regulatory behaviors of older drivers. Annu Proc Assoc Adv Automot Med. 2003;47:181–94. [PMC free article] [PubMed]
19. Man-Son-Hing M, Marshall SC, Molnar FJ, et al. Systematic review of driving risk and the efficacy of compensatory strategies in persons with dementia. J Am Geriatr Soc. 2007;55(6):878–84.[PubMed]
20. West CG, Gildengorin G, Haegerstrom-Portnoy G, et al. Vision and driving self-restriction in older adults. J Am Geriatr Soc. 2003;51(10):1348–55. [PubMed]
21. McGwin G, Jr, Sims RV, Pulley L, et al. Relations among chronic medical conditions, medications, and automobile crashes in the elderly: a population-based case-control study. Am J Epidemiol.2000;152(5):424–31. [PubMed]
22. Shah MN, Rathouz PJ, Chin MH. Emergency department utilization by noninstitutionalized elders. Acad Emerg Med. 2001 Mar;8(3):267–73. [PubMed]
23. Stiffler KA, Gerson LW. Health promotion and disease prevention in the emergency department.Emerg Med Clin North Am. 2006;24(4):849–69. [PubMed]
24. Llovera I, Ward MF, Ryan JG, et al. A survey of the emergency department population and their interest in preventive health education. Acad Emerg Med. 2003;10(2):155–60. [PubMed]
25. Parker D, McDonald L, Rabbitt P, et al. Elderly drivers and their accidents: the Aging Driver Questionnaire. Accid Anal Prev. 2000;32(6):751–9. [PubMed]
26. Molnar FJ, Byszewski AM, Marshall SC, et al. In-office evaluation of medical fitness to drive: practical approaches for assessing older people. Can Fam Physician. 2005;51:372–9.[PMC free article] [PubMed]
27. Janke M. Mature driver improvement program in California Transportation Research Record, National Research Council. 1994. pp. 77–83.
28. Marottoli RA, Ness PH, Araujo KL, et al. A randomized trial of an education program to enhance older driver performance. J Gerontol A Biol Sci Med Sci. 2007;62(10):1113–9. [PubMed]
29. McKnight AJ, Simmone GA, Weidman JR. National Public Service Institute, National Highway Traffic Safety Institute; 1982. Elderly Driver Retraining. DOT-HS-806 336.
30. Ragland DR, Satariano WA, MacLeod KE. Reasons given by older people for limitation or avoidance of driving. Gerontologist. 2004;44(2):237–44. [PubMed]
31. National Highway Traffic Safety Administration, Department of Transportation (US) Washington (DC): NHTSA; 2007. Traffic Safety Facts 2007. Available at: http://www-nrd.nhtsa.dot.gov/Pubs/TSF2007FE.PDF. Accessed September 1, 2009.
32. Fain MJ. Should older drivers have to prove that they are able to drive? Arch Intern Med.2003;163(18):2126–8. discussion 2132. [PubMed]
33. Fitten LJ. Driver screening for older adults. Arch Intern Med. 2003;163(18):2129–31. discussion 2131. [PubMed]
34. Byszewski AM, Graham ID, Amos S, et al. A continuing medical education initiative for Canadian primary care physicians: the driving and dementia toolkit: a pre- and postevaluation of knowledge, confidence gained, and satisfaction. J Am Geriatr Soc. 2003;51(10):1484–9. [PubMed]
35. Carr D, Schmader K, Bergman C, et al. A multidisciplinary approach in the evaluation of demented drivers referred to geriatric assessment centers. J Am Geriatr Soc. 1991;39(11):1132–6.[PubMed]
36. Li I, Smith R. Driving and the Elderly. Clinical Geriatrics. 2003;11(5):40–46.
37. Bogner HR, Straton JB, Gallo JJ, et al. The role of physicians in assessing older drivers: barriers, opportunities, and strategies. J Am Board Fam Pract. 2004;17(1):38–43. [PMC free article][PubMed]