Volume 16, Issue 7, December 2015.
Kelsey P. Mayrand, BS, et al.
Introduction: Current resuscitation guidelines emphasize a systems approach with a strong
emphasis on quality cardiopulmonary resuscitation (CPR). Despite the American Heart Association
(AHA) emphasis on quality CPR for over 10 years, resuscitation teams do not consistently meet
recommended CPR standards. The objective is to assess the impact on chest compression depth of
factors including bed height, step stool utilization, position of the rescuer’s arms and shoulders relative
to the point of chest compression, and rescuer characteristics including height, weight, and gender.
Methods: Fifty-six eligible subjects, including physician assistant students and first-year emergency
medicine residents, were enrolled and randomized to intervention (bed lowered and step stool
readily available) and control (bed raised and step stool accessible, but concealed) groups. We
instructed all subjects to complete all interventions on a high-fidelity mannequin per AHA guidelines.
Secondary end points included subject arm angle, height, weight group, and gender.
Results: Using an intention to treat analysis, the mean compression depths for the intervention
and control groups were not significantly different. Subjects positioning their arms at a 90-degree
angle relative to the sagittal plane of the mannequin’s chest achieved a mean compression
depth significantly greater than those compressing at an angle less than 90 degrees. There was
a significant correlation between using a step stool and achieving the correct shoulder position.
Subject height, weight group, and gender were all independently associated with compression depth.
Conclusion: Rescuer arm position relative to the patient’s chest and step stool utilization during
CPR are modifiable factors facilitating improved chest compression depth.
Volume 16, Issue 7, December 2015.
Jesse Z. Kellar, MD, et al.
The call from the nursing home relayed that an 85-yearold
male was coming in by ambulance complaining of
increased shortness of breath. The nursing home told us that
he had an unknown code status. Once the patient arrived, it
was clear that he was in the process of dying. While I was
preparing for aggressive resuscitative efforts, my attending
physician was shuffling through some paperwork that came
with the patient and discovered a “do not resuscitate” order,
signed by the patient. The paperwork also stated that he had
advanced cancer. It was clear why the patient had previously
decided he did not want any procedures to be done, which
we were quickly prepping to perform. With this added
information we put a stop to our efforts, followed the wishes
of the patient, and made him as comfortable as possible in his
final moments.
Volume 16, Issue 7, December 2015.
Anne M. Hakenewerth, PhD, et al.
Introduction: We analyzed emergency department (ED) visits by patients with mental health disorders
(MHDs) in North Carolina from 2008-2010 to determine frequencies and characteristics of ED visits by
older adults with MHDs.
Methods: We extracted ED visit data from the North Carolina Disease Event Tracking and Epidemiologic
Collection Tool (NC DETECT). We defined mental health visits as visits with a mental health ICD-9-CM
diagnostic code, and organized MHDs into clinically similar groups for analysis.
Results: Those ≥65 with MHDs accounted for 27.3% of all MHD ED visits, and 51.2% were admitted. The
most common MHD diagnoses for this age group were psychosis, and stress/anxiety/depression.
Conclusion: Older adults with MHDs account for over one-quarter of ED patients with MHDs, and their
numbers will continue to increase as the “boomer” population ages. We must anticipate and prepare for
the MHD-related needs of the elderly.
Volume 16, Issue 7, December 2015.
Namkee G. Choi, PhD, et al.
Introduction: Late middle-aged and older adults’ share of emergency department (ED) visits is increasing
more than other age groups. ED visits by individuals with substance-related problems are also increasing.
This paper was intended to identify subgroups of individuals aged 50+ by their risk for ED visits by
examining their health/mental health status and alcohol use patterns.
Methods: Data came from the 2013 National Health Interview Survey’s Sample Adult file (n=15,713).
Following descriptive analysis of sample characteristics by alcohol use patterns, latent class analysis
(LCA) modeling was fit using alcohol use pattern (lifetime abstainers, ex-drinkers, current infrequent/light/
moderate drinkers, and current heavy drinkers), chronic health and mental health status, and past-year
ED visits as indicators.
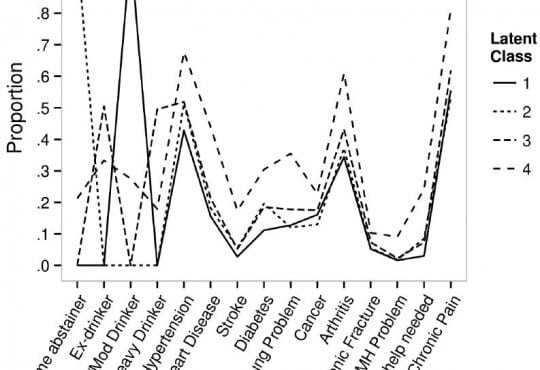
Results: LCA identified a four-class model. All members of Class 1 (35% of the sample; lowest-risk
group) were infrequent/light/moderate drinkers and exhibited the lowest probabilities of chronic health/
mental health problems; Class 2 (21%; low-risk group) consisted entirely of lifetime abstainers and,
despite being the oldest group, exhibited low probabilities of health/mental health problems; Class 3
(37%; moderate-risk group) was evenly divided between ex-drinkers and heavy drinkers; and Class 4
(7%; high-risk group) included all four groups of drinkers but more ex-drinkers. In addition, Class 4 had
the highest probabilities of chronic health/mental problems, unhealthy behaviors, and repeat ED visits,
with the highest proportion of Blacks and the lowest proportions of college graduates and employed
persons, indicating significant roles of these risk factors.
Conclusion: Alcohol nonuse/use (and quantity of use) and chronic health conditions are significant
contributors to varying levels of ED visit risk. Clinicians need to help heavy-drinking older adults reduce
unhealthy alcohol consumption and help both heavy drinkers and ex-drinkers improve chronic illnesses
self-management.
Volume 16, Issue 7, December 2015.
Luan E. Lawson, MD, MAEd, et al.
Introduction: Assessment of medical students’ knowledge in clinical settings is complex yet
essential to the learning process. Clinical clerkships use various types of written examinations to
objectively test medical knowledge within a given discipline. Within emergency medicine (EM), a new
national standardized exam was developed to test medical knowledge in this specialty. Evaluation
of the psychometric properties of a new examination is an important issue to address during test
development and use. Studies have shown that student performance on selected standardized
exams will reveal students’ strengths and/or weaknesses, so that effective remedial efforts can be
implemented. Our study sought to address these issues by examining the association of scores on
the new EM national exam with other standardized exam scores.
Methods: From August 2011 to April 2013, average National EM M4 examination scores of fourthyear
medical students taken at the end of a required EM clerkship were compiled. We examined
the correlation of the National EM M4 examination with the scores of initial attempts of the United
States Medical Licensing Exam (USMLE) Step 1 and Step 2 Clinical Knowledge (CK) examinations.
Correlation coefficients and 95% confidence intervals of correlation coefficients are reported. We
also examined the association between the national EM M4 examination score, final grades for the
EM rotation, and USMLE Step 1 and Step 2 CK scores.
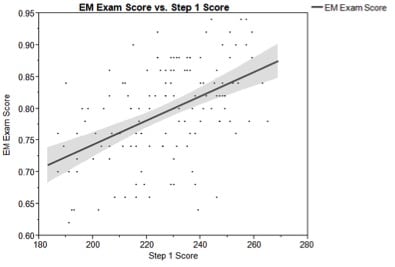
Results: 133 students were included in the study and achieved a mean score of 79.5 SD 8.0 on
the National EM M4 exam compared to a national mean of 79.7 SD 3.89. The mean USMLE Step
1 score was 226.8 SD 19.3. The mean USMLE Step 2 CK score was 238.5 SD 18.9. National EM
M4 examination scores showed moderate correlation with both USMLE Step 1 (mean score=226.8;
correlation coefficient=0.50; 95% CI [0.28-0.67]) and USMLE Step 2 CK (mean score=238.5;
correlation coefficient=0.47; 95% CI [0.25-0.65]). Students scoring below the median on the national
EM M4 exam also scored well below their colleagues on USMLE exams.
Conclusion: The moderate correlation of the national EM M4 examination and USMLE Step 1 and
Step 2 CK scores provides support for the utilization of the CDEM National EM M4 examination as
an effective means of assessing medical knowledge for fourth-year medical students. Identification of
students scoring lower on standardized exams allows for effective remedial efforts to be undertaken
throughout the medical education process.
Volume 16, Issue 7, December 2015.
Kevin R. Schwartz, MD, et al.
Introduction: Increasingly, pediatric and emergency medicine (EM) residents are pursuing clinical
rotations in low-income countries. Optimal pre-departure preparation for such rotations has not yet been
established. High-fidelity simulation represents a potentially effective modality for such preparation. This
study was designed to assess whether a pre-departure high-fidelity medical simulation curriculum is
effective in helping to prepare residents for clinical rotations in a low-income country.
Methods: 43 pediatric and EM residents planning clinical rotations in Liberia, West Africa, participated in a
simulation-based curriculum focused on severe pediatric malaria and malnutrition and were then assessed
by survey at three time points: pre-simulation, post-simulation, and after returning from work abroad.
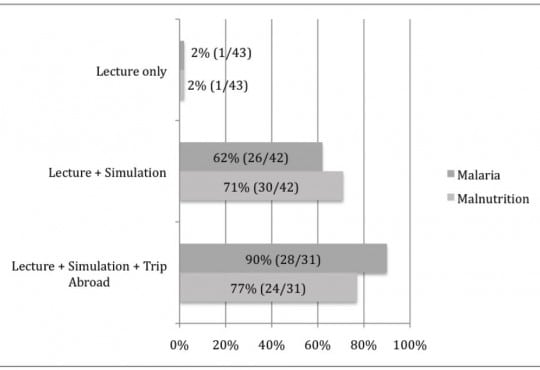
Results: Prior to simulation, 1/43 (2%) participants reported they were comfortable with the diagnosis
and management of severe malnutrition; this increased to 30/42 (71%) after simulation and 24/31 (77%)
after working abroad. Prior to simulation, 1/43 (2%) of residents reported comfort with the diagnosis and
management of severe malaria; this increased to 26/42 (62%) after simulation and 28/31 (90%) after
working abroad; 36/42 (86%) of residents agreed that a simulation-based global health curriculum is more
useful than a didactic curriculum alone, and 41/42 (98%) felt a simulator-based curriculum should be
offered to all residents planning a clinical trip to a low-income country.
Conclusion: High-fidelity simulation is effective in increasing residents’ self-rated comfort in management
of pediatric malaria and malnutrition and a majority of participating residents feel it should be included as
a component of pre-departure training for all residents rotating clinically to low-income countries.
Volume 16, Issue 7, December 2015.
Tara Murphy, et al.
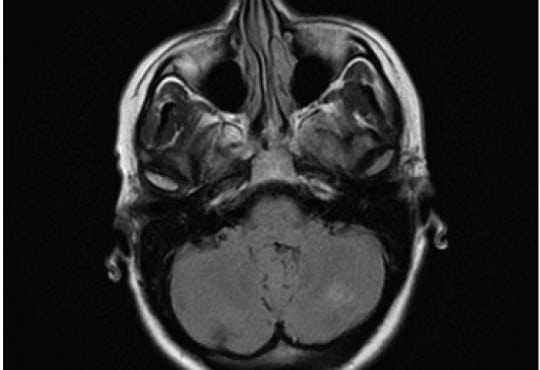
Posterior reversible encephalopathy syndrome (PRES) is an unusual condition typified by acute
visual impairment caused by sudden, marked parieto-occipital vasogenic edema. Thought to be
inflammatory in origin, it has been described in patients undergoing chemotherapy, with autoimmune
disease, and in some infections. We report a case of PRES that occurred one week after an episode
of acute pancreatitis in an otherwise healthy 40-year-old female. There was progressive visual
impairment over a 24-hour period with almost complete visual loss, with characteristic findings on
magnetic resonance imaging. After treatment with steroids, the visual loss recovered. Clinicians
should retain an index of suspicion of this rare condition in patients with visual impairment after acute
pancreatitis.
Volume 16, Issue 7, December 2015.
Jesse Z. Kellar, MD, et al.
A 14-year-old African American male presented to the emergency department with worsening left
eye redness, swelling, and vision loss over the preceding three days. History was notable for similar
eye redness and swelling without vision loss four months earlier, which improved following a brief
course of prednisone. He endorsed mild eye irritation and tearing with bright lights. There was
no history of fever, respiratory symptoms or trauma. Mother was medicating patient with leftover
antibiotic eye drops x3 days without improvement. Physical examination on presentation notable
for proptosis of left eye, lid, and periorbital swelling, mild scleral injection, and central vision loss in
affected eye (20/200 OS, 20/25 OD). Extraocular movements and pupillary exam were normal. No
corneal fluorescein uptake, abnormal cell, flare, or siedel sign were seen during slit lamp exam. Eye
pressures were 24 mmHg in both eyes. Bedside ultrasonography was performed (Figure 1 showing
retinal detachment, Ultrasound Video 2 showing detachment in orbital scan).
Volume 16, Issue 7, December 2015.
Laura J. Fil, DO, et al.
Multiple sclerosis (MS) is an immune mediated inflammatory disease that attacks myelinated axons
in the central nervous system. Dalfampridine (4-aminopyridine) was approved by the Food and
Drug Administration in January 2010 for treatment of MS. Our patient was a 34-year-old male with a
history of MS, who was brought to the emergency department after being found unresponsive. His
current medications were valacyclovir, temazepam, dalfampridine (4-AP) and a tysabri intravenous
(IV) infusion. Fifteen minutes after arrival the patient seized. The seizures were refractory to
benzodiazepines, barbiturates and phenytoin. The 4-AP level was 530ng/mL (25ng/mL and 49ng/
mL). The patient stopped seizing on hospital day 3 and was discharged 14 days later with normal
mental status and neurologic exam. 4-AP is a potassium channel blocker that blocks the potassium
ion current of repolarization following an action potential. The blockade of the potassium channel at
the level of the membrane widens the action potential and enhances the release of acetylcholine,
thus increasing post-synaptic action potentials. The treatment of patients with 4-AP overdose is
supportive. Animal data suggest that patients with toxic levels of 4-AP may respond to phenytoin.
Our case illustrates the highest recorded level of 4-AP in an overdose. Our patient appeared to be
refractory to a combination of high doses of anticonvulsants and only improved with time.
Volume 16, Issue 7, December 2015.
Erik A. Berg, MD
A 60-year-old female with a history of
ventriculoperitoneal shunt (VPS) placement three years
prior presented with a painful abdominal wall mass.
The patient denied fevers, nausea, vomiting, headaches,
or dizziness. Physical exam revealed an afebrile, wellappearing
female with a raised, erythematous, fluctuant mass
on the right lower abdominal wall. She had no abdominal
tenderness otherwise. Labs were unremarkable. A bedside
ultrasound revealed a complex fluid collection over the
area of fluctuance that tracked along the course of the VPS
tubing into the abdomen. Plan for incision and drainage was
deferred. Neurosurgery was consulted. The neurosurgeon
attempted to tap the shunt but encountered very high
resistance. The patient was admitted for intravenous antibiotics for VPS infection and malfunction.
Volume 16, Issue 7, December 2015.
Sean P. Nordt, MD, PharmD, et al.
A 37-year-old male presented to the emergency
department (ED) in police custody for “medical clearance”
before being taken to jail. The patient was approached by
police officers for suspicion of selling illicit drugs. When
approached by police he ran away and was witnessed to
swallow several small plastic baggies suspected to contain
heroin. He was apprehended and brought to the ED.
On arrival, he was asymptomatic with a blood pressure
144/83mmHg, heart rate 67bpm, respiratory rate of 19bpm,
oxygen saturation of 99% on room air and afebrile. A Glasgow
coma score was 15 and he was alert and oriented to person,
place and time. Patient had a negative review of systems.
On physical examination pupils were 4mm and reactive to
light, lungs clear to auscultation and had normal respiratory
rate with normal cardiovascular exam. Abdomen was soft,
non-tender and non-distended with present bowel sounds.
The patient admitted to ingesting approximately 20 packets
of heroin to avoid being charged with possession. The patient
declined activated charcoal and whole bowel irrigation (WBI)
with polyethylene glycol-electrolyte solution (PEG-ELS). The
patient declined a urine toxicology immunoassay screen. A
computed tomography (CT) of his abdomen with contrast was
obtained and read as normal except for a cluster of foreign
bodies within the distal stomach likely contained within a
plastic bag.
Volume 16, Issue 7, December 2015.
Po-Jen Yang, MD, et al.
A previously healthy 27-year-old man presented to the
emergency department with a three-day history of left lower
quadrant pain. He denied fever, nausea, vomiting, or diarrhea.
Vital signs were unremarkable, and physical examination
revealed tenderness in the left iliac fossa without peritoneal
signs. His leukocyte count and C-reactive protein were slightly
elevated. On abdominal computed tomography (CT) (Figure),
a fatty ovoid mass abutting sigmoid colon demonstrated the
infarcted or inflamed appendix epiploica. A surrounding
hyperdense rim (hyperattenuating ring sign) represented the
inflamed visceral peritoneal covering, and the central linear
hyperdensity corresponded to the thrombosed central vessel.
Volume 16, Issue 7, December 2015.
Jonathan G. Wagner, MD, et al.
A 52-year-old African American male with a long history of poorly controlled hypertension presented
to the emergency department (ED) with two days of genital edema and pain. During ED work-up,
the patient developed sudden onset of non-pitting, non-pruritic, and non-urticarial upper lip edema.
Review of his antihypertensive medication list revealed that he normally took benazepril, highly
suggestive of a diagnosis of angiotensin-converting-enzyme inhibitor-related angioedema (ACEIRA).
We present the first reported case of penile ACEI-RA that progressed to involve the oropharynx.
The ED management of the condition and some of the newer treatment options available for ACEIRA
is also briefly discussed.
Volume 16, Issue 7, December 2015.
Leonieke Groot, MD, et al.
Introduction: Currently, it is common practice in the emergency department (ED) for pain relief
in hip-fracture patients to administer pain medication, commonly systemic opioids. However, with
these pain medications come a high risk of side effects, especially in elderly patients. This study
investigated the safety profile and success rate of fascia iliaca compartment block (FICB) in a
busy ED. This ED was staffed with emergency physicians (EPs) and residents of varying levels of
experience. This study followed patients’ pain levels at various hourly intervals up to eight hours
post procedure.
Methods: Between September 2012 and July 2013, we performed a prospective pilot study on
hip-fracture patients who were admitted to the ED of a teaching hospital in the Netherlands. These
patients were followed and evaluated post FICB for pain relief. Secondary outcome was the use of
opioids as rescue medication.
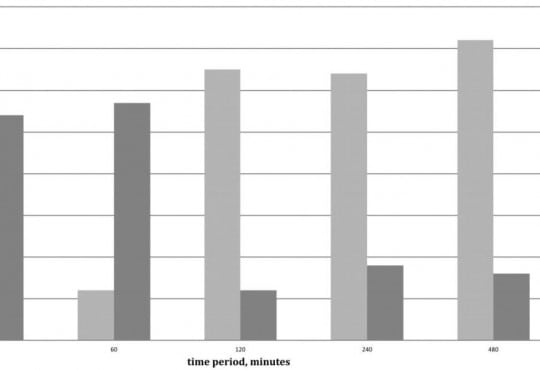
Results: Of the 43 patients in this study, patients overall experienced less pain after the FICB
(p=0.04). This reduction in pain was studied in conjunction with the use and non-use of opioids. A
clinically meaningful decrease in pain was achieved after 30 minutes in 62% of patients (54% with
the use of opioids, 8% without opioids); after 240 minutes in 82% of patients (18% with opioids, 64%
without opioids); after 480 minutes in 88% of patients (16% with opioids, 72% without opioids). No
adverse events were reported.
Conclusion: In a busy Dutch ED with rotating residents of varying levels of experience, FICB seems
to be an efficient, safe and practical method for pain reduction in patients with a hip fracture. Even
without the use of opioids, pain reduction was achieved in 64% of patients after four hours and in
72% of patients after eight hours.
Volume 16, Issue 7, December 2015.
Peter Moffett, MD, et al.
A 65-year-old male presented to the emergency department
complaining of two hours of severe lower abdominal
pain radiating into his left testicle. The patient described a
vascular procedure in the past but did not recall the details.
An emergent bedside ultrasound was performed to evaluate
the abdominal aorta. During the exam an echogenic object
consistent with a prior endovascular stent was discovered
in the distal aorta prompting further ultrasound evaluation
of the iliac artery (Figure). A true lumen (thin black arrow)
was visualized with evidence of leak (white arrows) during
color Doppler evaluation. The patient was taken emergently
to computed tomography and the diagnosis of an iliac artery
pseudoaneurysm from an endoleak was confirmed.
Volume 16, Issue 7, December 2015.
Brandon Fetterolf, DO, et al.
A 35-year-old male presented with lower gum
pain associated with fever, chills, and sore throat. His
medical history included intravenous drug use, human
immunodeficiency virus infection, and hepatitis C. Physical
exam revealed tachycardia, a temperature of 38.9°C, anterior
cervical lymphadenopathy, halitosis, an edematous lower lip,
and purulent ulcers anterior and posterior to lower central
incisors with marked tenderness and erythema (Figure).
His laboratory work was notable for a low white blood cell
count (2.6 thousand/µl), neutropenia (0.11 thousand/µl), a
low absolute CD4 lymphocyte count (0.5 thousand/µl), and
elevated C-reactive protein (129mg/L) and sedimentation
rate (23mm/hr). A computed tomography study showed a
0.5×1.3×0.3cm abscess anterior to the mandibular symphysis.
Volume 16, Issue 7, December 2015.
Sarah E. Frasure, MD, et al.
A 42-year-old female presented to the emergency
department with diffuse abdominal pain, vaginal discharge,
and a fever of 102°F. She described multiple recent male
sexual partners, with inconsistent condom use. Her vital
signs were unremarkable. Her physical exam was notable for
moderate right lower quadrant tenderness to palpation. There
was no cervical motion tenderness. The emergency physician
performed a bedside abdominal ultrasound (Video), and
subsequently ordered a computed tomography (Figure), which
confirmed the diagnosis.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 41-year-old female presented to the emergency
department with nausea, vomiting and foreign body sensation
in her throat. The patient had multiple co-morbidities including
hypertension, diabetes, cervical cancer and gastroparesis with
gastrojejunostomy (GJ) tube. The patient had stable vitals, was
in no respiratory distress, and her only complaint was mild throat
pain and abdominal pain at the GJ tube insertion site. Physical
exam revealed a foreign object in the oropharynx (Figure 1).
Abdominal exam showed a soft, non-distended, non-tender
abdomen with GJ-tube and colostomy in place. Abdominal series
and upright chest radiograph were obtained (Figure 2).
Volume 16, Issue 7, December 2015.
Marc A. Polacco, MD, et al.
Often discovered only after an extensive work up for hemoptysis and hematemesis, vallecular varices
are a rare cause of oral bleeding that increase patient morbidity due to delay of diagnosis.
We describe an 89-year-old male who presented with a week of intermittent oral blood production. A
vallecular varix was identified on fiberoptic laryngoscopy after studies for hematemesis and hemoptysis
had been performed, including negative esophagogastroduodenoscopy and bronchoscopy.
Awareness of this pathology and key points in the patient history can direct the clinician toward the
correct diagnosis, expediting treatment and limiting invasive diagnostic procedures for pulmonary or
gastric etiologies of bleeding.
Volume 16, Issue 7, December 2015.
Brian J. Wolk, MD
A 66-year-old female was transferred from an outside
hospital for possible ST segment elevation myocardial
infarction (STEMI). The patient reported feeling poorly for the
last day, with epigastric pain, nausea, and multiple episodes
of vomiting. Patient’s medical history was significant for
diabetes mellitus, hypertension, atrial fibrillation, and multiple
sclerosis. Electrocardiogram (EKG) was as noted (Figure).
Initial troponin was 0.14 (<0.03ng/mL). The patient was
taken emergently to the cardiac cath lab for possible posterior
STEMI. Angiogram demonstrated no significant evidence of
coronary artery disease, with an EF of 75%.
Volume 16, Issue 7, December 2015.
Lauren M. Porter, DO, et al.
A 42-year-old male was assisted from a car in front
of our inner city stand-alone emergency department (ED)
with a stab wound to the right chest. He was confused and
bleeding; his past medical history was unknown. The patient
was diaphoretic, pale and confused with a large vertical stab
wound over his right chest with no other obvious injuries.
On initial exam in the outlying ED, his back was obscured
by blood. He was transferred to the trauma center where
during a full secondary survey a 2cm wound was located over
the patient’s lumbar spine. The patient was stabilized and
taken for imaging. No focused assessment with sonography
for trauma (FAST) was done at either site; however, the
FAST exam, which emphasizes the search for extraluminal
blood, would not have been expected to find a foreign body
Volume 16, Issue 7, December 2015.
Krystal Garcia, BS, et al.
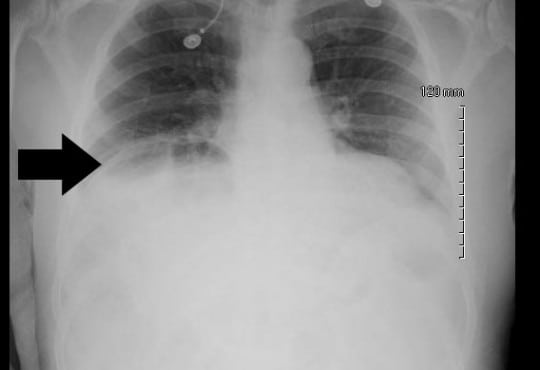
A 68-year-old male with a history of prostate cancer
presented with a two-day history of fever and left flank pain.
Vital signs included a temperature of 39.4 degrees Celsius with
93% oxygen saturation and heart rate of 112 beats per minute. An
upright chest radiograph showed concern for free intraperitoneal
air (Figure) with a white blood cell count of 17.3. A computed
tomography of the abdomen and pelvis revealed a Chilaiditi sign
with pyelonephritis, which was confirmed on urinalysis. He was
admitted for intravenous antibiotics.
Volume 16, Issue 7, December 2015.
Yudai Iwasaki, MD
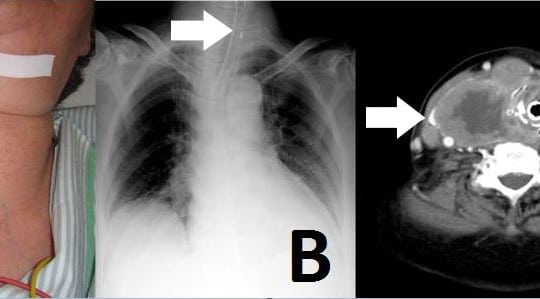
An 81-year-old woman was admitted to our emergency
department (ED) with neck swelling (Figure 1A) and
advancing dyspnea. Stridor was noted on auscultation of
her neck, and her breathing was labored. We immediately
diagnosed airway obstruction, and emergency intubation was
performed using a video laryngoscope (AWS-S100L®, Pentax
Corporation, Tokyo, Japan). The epiglottis was found to have
shifted to the left on chest video images and chest radiograph.
{kind=link}