{kind=link}

Archives
Emergency Department Access
Examining the Effect of the Affordable Care Act on Two Illinois Emergency Departments
Westjem Read More
Emergency Department Access
A Geospatial Analysis of Freestanding and Hospital Emergency Department Accessibility via Public Transit
Westjem Read More
Emergency Department Access
Impact of Superstorm Sandy on Medicare Patients’ Utilization of Hospitals and Emergency Departments
Westjem Read More
Emergency Department Access
Prevalence of Homelessness in the Emergency Department Setting
Westjem Read More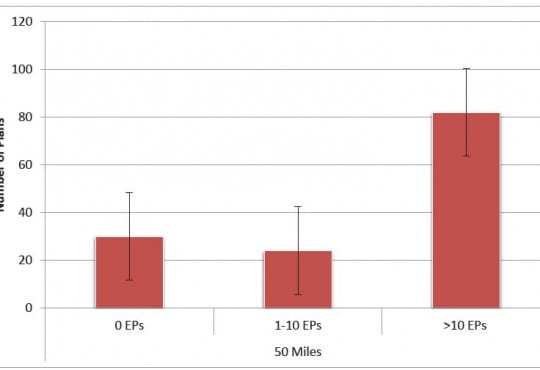
Emergency Department Access
Association of Insurance Status with Severity and Management in ED Patients with Asthma Exacerbation
Westjem Read More
Emergency Department Access
Rural Ambulatory Access for Semi-Urgent Care and the Relationship of Distance to an Emergency Department
Westjem Read More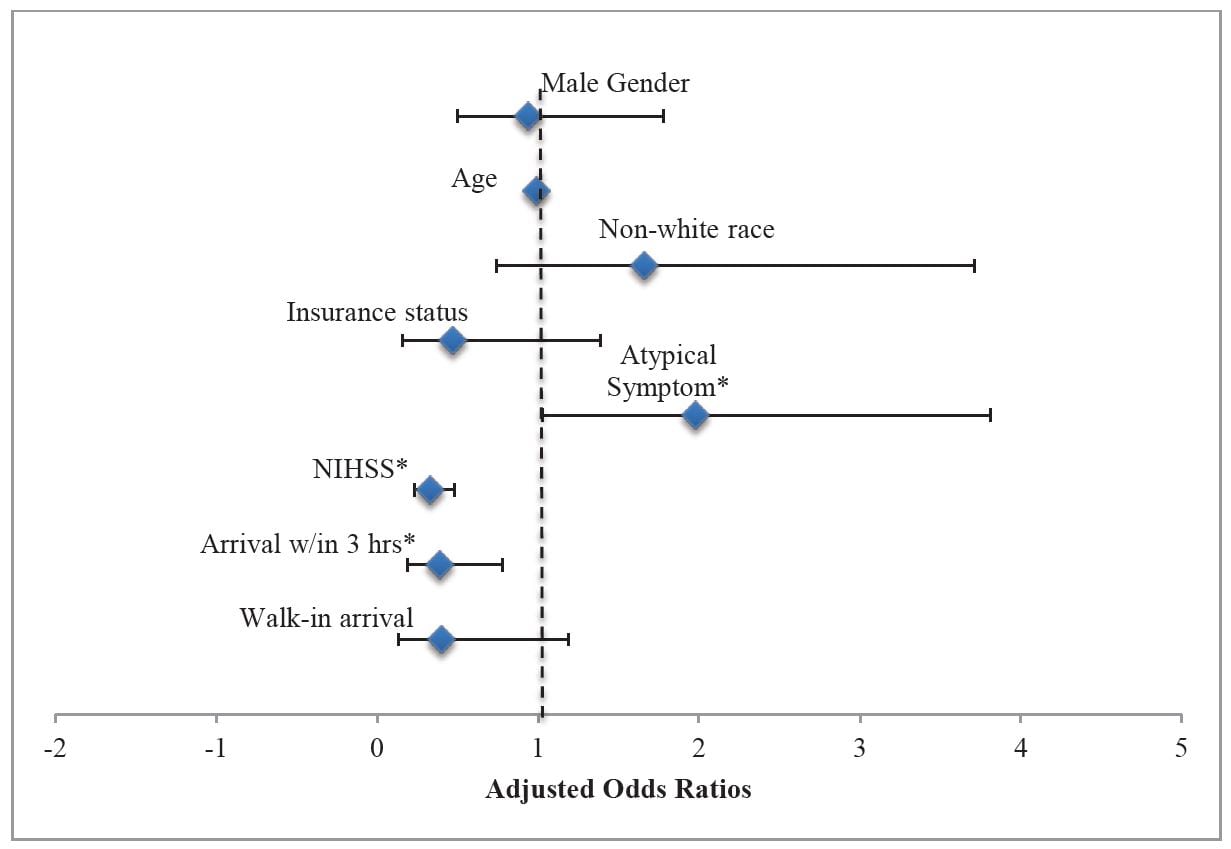
Emergency Department Access
Lack of Gender Disparities in Emergency Department Triage of Acute Stroke Patients
Westjem Read More
Emergency Department Access
Exploring Real-time Patient Decision-making for Acute Care: A Pilot Study
WestJEM Read More
Emergency Department Access
National Study of Non-urgent Emergency Department Visits and Associated Resource Utilization
WestJEM Read More
Emergency Department Access Healthcare Utilization
New Drugs and Devices from 2011 – 2012 That Might Change Your Practice
WestJEM Read More
Emergency Department Access
Emergency Department Crowding and Time to Antibiotic Administration in Febrile Infants
WestJEM Read More
Emergency Department Access
Established and Novel Initiatives to Reduce Crowding in Emergency Departments
WestJEM Read More
Emergency Department Access