{kind=link}

Emergency Department Access
Emergency Department Access
Examining the Effect of the Affordable Care Act on Two Illinois Emergency Departments
Westjem Read More
Emergency Department Access
A Geospatial Analysis of Freestanding and Hospital Emergency Department Accessibility via Public Transit
Westjem Read More
Emergency Department Access
Impact of Superstorm Sandy on Medicare Patients’ Utilization of Hospitals and Emergency Departments
Westjem Read More
Emergency Department Access
Prevalence of Homelessness in the Emergency Department Setting
Westjem Read More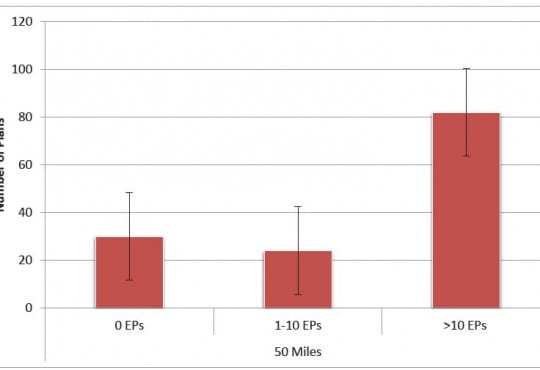
Emergency Department Access
Association of Insurance Status with Severity and Management in ED Patients with Asthma Exacerbation
Westjem Read More
Emergency Department Access
Rural Ambulatory Access for Semi-Urgent Care and the Relationship of Distance to an Emergency Department
Westjem Read More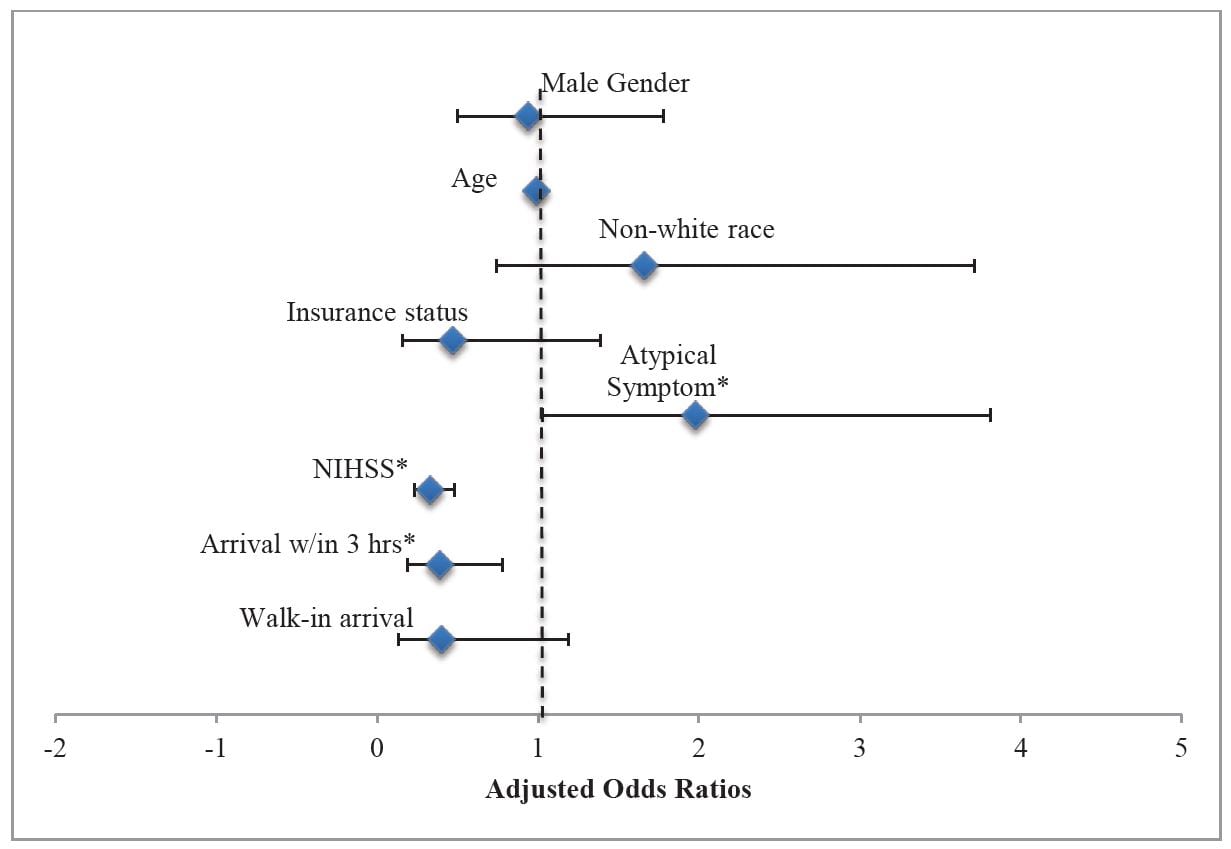
Emergency Department Access
Lack of Gender Disparities in Emergency Department Triage of Acute Stroke Patients
Westjem Read More
Emergency Department Access