
{kind=link}
| Author | Affiliation |
|---|---|
| Shanda Gomes | University of California, Irvine School of Medicine |
| Scott Rudkin, MD, MBA | University of California, Irvine School of Medicine |
| Fong Tsai, MD | University of California, Irvine School of Medicine |
| Shahram Lotfipour, MD, MPH | University of California, Irvine School of Medicine |
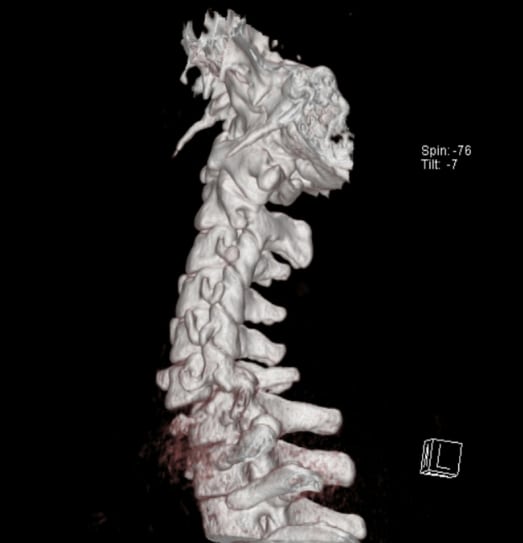
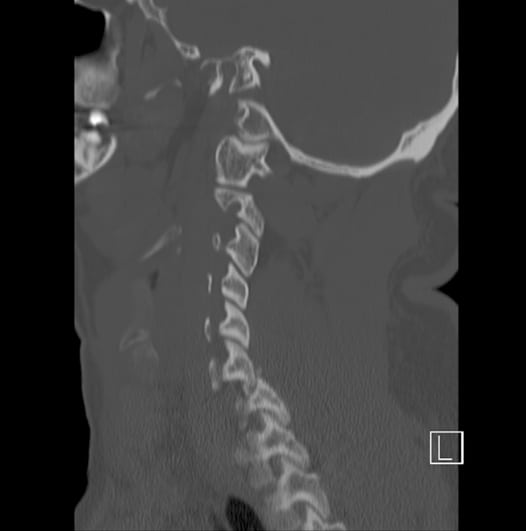
An intoxicated 29-year-old male presented to the emergency department after diving into a pool with reported loss of consciousness and complaining of neck pain. On arrival the Glasgow Coma Scale was 15 and vital signs were unremarkable. Physical exam was significant for focal C6 tenderness without step-off deformity, decreased grip strength, biceps hyperreflexia and absent triceps reflexes bilaterally. Lower extremities demonstrated flaccid paralysis, loss of sensation from the T4 dermatome down, urinary retention and no rectal tone. Cervical spine computed tomography (CT) demonstrated bilateral fractured and dislocated facets C6 on C7. The patient was treated with intravenous methylprednisolone and admitted to the Neurosurgical Intensive Care Unit, after undergoing C6–C7 anterior disk excision with subsequent posterior fusion. At discharge he had a C7 functional level with mixed motor deficits inferiorly.
Bilateral facet dislocation occurs when a vertebra’s inferior facet dislocates anteriorly over the lower vertebra’s superior facet, locking in the intervertebral foramens, creating a severely unstable fracture.2,3 CT has a higher sensitivity for C-spine injury and is the preferred imaging modality.2 Sagittal reconstructions best identify the dislocated, locked facets; axial views can demonstrate a “reverse-hamburger-bun sign.”2 While facet dislocation injuries are rare, representing less than 10% of C-spine injuries, the neurologic morbidity is tragically high.1,3 Common mechanisms for this injury include motor vehicle collisions (61%) and diving accidents (15%), where extreme flexion and axial loading occur. 1 Ivancic et al.3 reported that the dynamic narrowing of the spinal canal during the dislocation is sevenfold greater than the narrowing observed in the canal immediately post dislocation; thus, CT images may under-appreciate the extent of the injury. Complete spinal cord injury is not uncommon.1,2
Footnotes
Thank you to Jaspret Brar, MD for aiding with the identification and selection of images.
Supervising Section Editor: Rick A. McPheeters, DO
Submission history: Submitted August 20, 2008; Revision Received September 09, 2008; Accepted September 12, 2008.
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for correspondence: Shahram Lotfipour, MD, MPH. Department of Emergency Medicine, 101 The City Drive, Rte 128-01, Orange, CA 92868
Email: SHL@uci.edu
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Hadley, Fitzpatrick, Sonntag, Browner Facet fracture-dislocation injuries of the cervical. Neurosurgery. 1992;30:661–666. [PubMed]
2. Daffner, Daffner CT diagnosis of facet dislocations: The “Hamburger Bun” and “Reverse Hamburger Bun” signs. JEM. 2002;23:387–394.
3. Ivancic, Pearson, Tominaga, et al. Mechanism of cervical spinal cord injury during bilateral facet dislocation. Spine. 2007;15(32):2467–2473. [PubMed]
{kind=link}