
{kind=link}
| Author | Affiliation |
|---|---|
| Annalee Baker, MD | New York University, New York, NY |
| Sosamma T. Methratta, MD | New York University, New York, NY |
| Arabinda K. Choudhary, MD | New York University, New York, NY |
An 18-hour-old neonate was found to have absent movement of the left arm and a mildly edematous elbow following precipitous delivery with observed traction applied to the left arm. Radiographs (Figure 1) showed abnormal elbow alignment without osseous fracture and a moderate joint effusion. Magnetic resonance imaging (MRI) [Figure 2] revealed a transverse fracture through the distal left humeral physis with posterior displacement of the distal cartilaginous epiphysis. An orthopedic surgeon placed the patient in a long arm splint with the arm at 90° of flexion and pronation to align the transphyseal fracture. One week later the splint was removed. The fingers and hand appeared to move normally, but left shoulder movement was persistently decreased, thought secondary to a brachial plexus stretch injury.

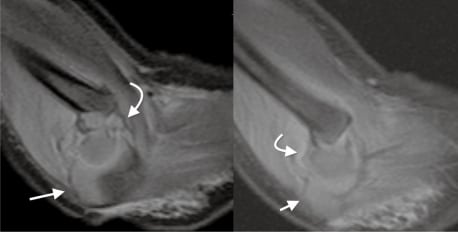
Traumatic separation of the neonatal distal humeral epiphysis is a rare injury, usually due to birth trauma or occasionally child abuse.1 Clinical findings include elbow swelling, muffled crepitus and pseudo paralysis of the extremity.1 Evaluation with plain radiography may be challenging and give the spurious appearance of dislocation until the capitellar ossification center had developed, usually around three to nine months of age.2 MRI may be achieved without sedation in neonates. It is accurate and will provide definitive diagnosis with good visualization of the cartilage, bone and soft tissue in multiple planes.2 Treatment involves casting, usually with closed reduction if the injury is detected early.1
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted June 4, 2010; Revision received July 20, 2010; Accepted August 23, 2010
Reprints available through open access at http://escholarship.org/uc/uciem_westjem.
Address for Correspondence: Annalee Baker, 235 E 10th St Apt B, New York, NY 10003
Email: annalee.baker@gmail.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Jacobsen S, Hansson G, Nathorst J. Traumatic separation of the distal epiphysis of the humerus sustained at birth. J Bone Joint Surg Br. 2009;91:797–802. [PubMed]
2. Sawant MR, Narayanan S, O’Neill K, et al. Distal humeral epiphysis fracture separation in neonates—diagnosis using MRI scan. Injury. 2002;33:179–81. [PubMed]
{kind=link}