Traumatic injuries to the knee are common in emergency medicine. Bedside ultrasound (US) has benefits in the rapid initial detection of injuries to the patella. In addition, US can also quickly detect injuries to the entire knee extensor mechanism, including the quadriceps tendon and inferior patellar ligament, which may be difficult to diagnose with plain radiographs.
We describe the use of point-of-care ultrasound to localize a retained intravenous drug needle, and subsequent surgical removal without computed tomography.
Identification and retrieval of soft-tissue foreign bodies (STFB) poses significant challenges in the emergency department. Prior studies have demonstrated the utility of ultrasound (US) in identification and retrieval of STFBs, including radiolucent objects such as wood. We present a case of STFB extraction that uses US to identify the longitudinal axis of the object. With the longitudinal axis identified, the foreign body can be excised by making an incision where the foreign body is closest to the skin. The importance of this technique as it pertains to minimizing surrounding tissue destruction and discomfort for patients has not been previously reported.
We describe a case where a patient presented with acute angiotensin-converting enzyme inhibitor (ACE-I) induced angioedema without signs or symptoms of upper airway edema beyond lip swelling. Point-of-care ultrasound (POCUS) was used as an initial diagnostic test and identified left-sided subglottic upper airway edema that was immediately confirmed with indirect fiberoptic laryngoscopy. ACE-I induced angioedema and the historical use of ultrasound in evaluation of the upper airway is briefly discussed. To our knowledge, POCUS has not been used to identify acute upper airway edema in the emergency setting. Further investigation is needed to determine if POCUS is a sensitive and specific-enough tool for the identification and evaluation of acute upper airway edema.
An 11-year-old previously healthy girl presented to the emergency department (ED) with three weeks of a rapidly progressive swelling underneath her tongue, causing difficulty in talking and eating. Physical examination revealed a 4.5 × 3 cm sublingual mass arising from the base of the tongue, around the midline (Figure 1). The mass was soft, movable and non-tender. The contents had a bluish hue, which was covered with normal appearing mucosa. A point-of-care ultrasound (POCUS) revealed a well-circumscribed homogenous cystic mass, separated from the muscular fibers of the tongue, without extravasation towards the neck (Figure 2) and without intra-cystic flow. A diagnosis of simple ranula was made.
Mobile COWs (Computer on Wheels): Hamburger or VEAL?
Maxwell Jen, MD, et al.
The HITECH (Health Information Technology for Economic and Clinical Health) Act of 2009 galvanized the universal adoption of electronic health record (EHR) systems to improve the quality, delivery, and coordination of patient care.1 Initial results demonstrated improvement in population health outcomes and increased transparency.2-3 Through the HITECH Act’s Meaningful Use (MU) incentives, EHR adoption also promised shorter hospital stays, reduced costs and improved access to healthcare data.4 These promises, however, never materialized; studies have demonstrated that EHR adoption causes decreased rates of patients seen per hour, highly variable documentation times, and increased order entry times.
Optic Nerve Sheath Diameter Measurement During Diabetic Ketoacidosis: A Pilot Study
Bergmann, DO, MS, et al.
Diabetic ketoacidosis-related cerebral edema (DKA-CE) occurs in up to 1% of children with type 1 diabetes (T1D),1 with approximately 20% displaying neurologic symptoms at presentation.2,3 Similarly, up to 54% have a mild form of subclinical DKA-CE identified by extracellular fluid measurements on magnetic resonance imaging (MRI), which is associated with alterations in neuronal function and cerebral injury on MR spectroscopy.2-6 This suggests that DKA-CE occurs along a continuum, ranging from asymptomatic imaging changes, mild neurologic injury, to cerebral herniation and death.
Volume 17, Issue 2, March 2016.
Warren Wiechmann, MD, MBA, et al.
Introduction: The use of personal mobile devices in the medical field has grown quickly, and a large
proportion of physicians use their mobile devices as an immediate resource for clinical decisionmaking,
prescription information and other medical information. The iTunes App Store (Apple,
Inc.) contains approximately 20,000 apps in its “Medical” category, providing a robust repository
of resources for clinicians; however, this represents only 2% of the entire App Store. The App
Store does not have strict criteria for identifying content specific to practicing physicians, making
the identification of clinically relevant content difficult. The objective of this study is to quantify
the characteristics of existing medical applications in the iTunes App Store that could be used by
emergency physicians, residents, or medical students.
Methods: We found applications related to emergency medicine (EM) by searching the iTunes App
Store for 21 terms representing core content areas of EM, such as “emergency medicine,” “critical
care,” “orthopedics,” and “procedures.” Two physicians independently reviewed descriptions of
these applications in the App Store and categorized each as the following: Clinically Relevant, Book/
Published Source, Non-English, Study Tools, or Not Relevant. A third physician reviewer resolved
disagreements about categorization. Descriptive statistics were calculated.
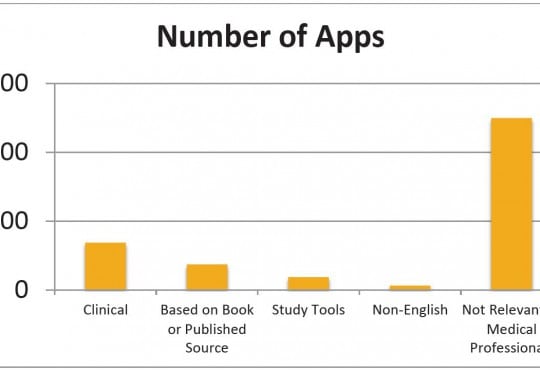
Results: We found a total of 7,699 apps from the 21 search terms, of which 17.8% were clinical,
9.6% were based on a book or published source, 1.6% were non-English, 0.7% were clinically
relevant patient education resources, and 4.8% were study tools. Most significantly, 64.9% were
considered not relevant to medical professionals. Clinically relevant apps make up approximately
6.9% of the App Store’s “Medical” Category and 0.1% of the overall App Store.
Conclusion: Clinically relevant apps represent only a small percentage (6.9%) of the total App
volume within the Medical section of the App Store. Without a structured search-and-evaluation
strategy, it may be difficult for the casual user to identify this potentially useful content. Given the
increasing adoption of devices in healthcare, national EM associations should consider curating
these resources for their members.
Volume 17, Issue 2, March 2016.
Michael T. Long, MD
A 16-year-old male presented with three months of
palpitations at rest, fatigue, and episodic pre-syncope; his
paternal grandfather died following presumed premature
myocardial infarction at age 30. He was seen and discharged
one week previously at an outside emergency department
(ED). He followed up with his pediatrician and was promptly
referred to our pediatric ED for evaluation given his risk factors.
Pertinent vitals on arrival were pulse 110, blood pressure
129/66, and oxygen saturation 97% on room air. His exam
was remarkable for a left upper sternal border 2/6 holosystolic
murmur with radiation to apex. In addition, the patient had a
chest radiograph (Figure), a nonspecific but abnormal EKG, and
a point-of-care ultrasound (POCUS) of the heart performed.
Volume 17, Issue 2, March 2016.
Bradley Jacobsen, BS, et al.
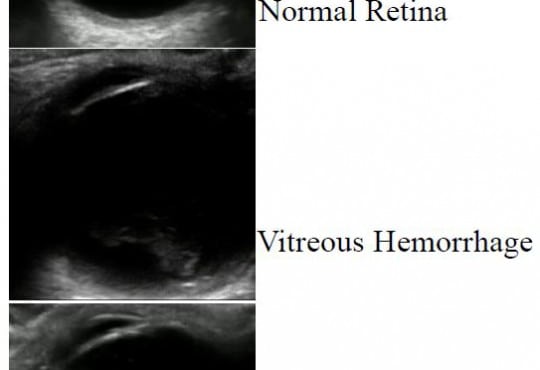
Introduction: Retinal detachment is an ocular emergency that commonly presents to the
emergency department (ED). Ophthalmologists are able to accurately make this diagnosis with a
dilated fundoscopic exam, scleral depression or ophthalmic ultrasound when a view to the retina is
obstructed. Emergency physicians (EPs) are not trained to examine the peripheral retina, and thus
ophthalmic ultrasound can be used to aid in diagnosis. We assessed the accuracy of ocular point-ofcare
ultrasound (POCUS) in diagnosing retinal detachment.
Methods: We retrospectively reviewed charts of ED patients with suspected retinal detachment
who underwent ocular POCUS between July 2012 and May 2015. Charts were reviewed for
patients presenting to the ED with ocular complaints and clinical concern for retinal detachment.
We compared ocular POCUS performed by EPs against the criterion reference of the consulting
ophthalmologist’s diagnosis.
Results: We enrolled a total of 109 patients. Of the 34 patients diagnosed with retinal detachment
by the ophthalmologists, 31 were correctly identified as having retinal detachment by the EP using
ocular POCUS. Of the 75 patients who did not have retinal detachment, 72 were ruled out by ocular
POCUS by the EP. This resulted in a POCUS sensitivity of 91% (95% CI [76-98]) and specificity of
96% (95% CI [89-99]).
Conclusion: This retrospective study suggests that ocular POCUS performed by EPs can aid in the
diagnosis of retinal detachment in ED.
Volume 17, Issue 2, March 2016.
Tony Zitek, MD, et al.
Introduction: Two-point compression ultrasound is purportedly a simple and accurate means to
diagnose proximal lower extremity deep vein thrombosis (DVT), but the pitfalls of this technique
have not been fully elucidated. The objective of this study is to determine the accuracy of emergency
medicine resident-performed two-point compression ultrasound, and to determine what technical
errors are commonly made by novice ultrasonographers using this technique.
Methods: This was a prospective diagnostic test assessment of a convenience sample of adult
emergency department (ED) patients suspected of having a lower extremity DVT. After brief training
on the technique, residents performed two-point compression ultrasounds on enrolled patients.
Subsequently a radiology department ultrasound was performed and used as the gold standard.
Residents were instructed to save videos of their ultrasounds for technical analysis.
Results: Overall, 288 two-point compression ultrasound studies were performed. There were 28
cases that were deemed to be positive for DVT by radiology ultrasound. Among these 28, 16 were
identified by the residents with two-point compression. Among the 260 cases deemed to be negative
for DVT by radiology ultrasound, 10 were thought to be positive by the residents using two-point
compression. This led to a sensitivity of 57.1% (95% CI [38.8-75.5]) and a specificity of 96.1% (95%
CI [93.8-98.5]) for resident-performed two-point compression ultrasound. This corresponds to a
positive predictive value of 61.5% (95% CI [42.8-80.2]) and a negative predictive value of 95.4%
(95% CI [92.9-98.0]). The positive likelihood ratio is 14.9 (95% CI [7.5-29.5]) and the negative
likelihood ratio is 0.45 (95% CI [0.29-0.68]). Video analysis revealed that in four cases the resident
did not identify a DVT because the thrombus was isolated to the superior femoral vein (SFV), which
is not evaluated by two-point compression. Moreover, the video analysis revealed that the most
common mistake made by the residents was inadequate visualization of the popliteal vein.
Conclusion: Two-point compression ultrasound does not identify isolated SFV thrombi, which
reduces its sensitivity. Moreover, this technique may be more difficult than previously reported, in
part because novice ultrasonographers have difficulty properly assessing the popliteal vein.
Volume 17, Issue 2, March 2016.
Shane M. Summers, MD, RDMS, et al.
Introduction: Bedside thoracic ultrasound (US) can rapidly diagnose pneumothorax (PTX) with
improved accuracy over the physical examination and without the need for chest radiography (CXR);
however, US is highly operator dependent. A computerized diagnostic assistant was developed
by the United States Army Institute of Surgical Research to detect PTX on standard thoracic US
images. This computer algorithm is designed to automatically detect sonographic signs of PTX
by systematically analyzing B-mode US video clips for pleural sliding and M-mode still images for
the seashore sign. This was a pilot study to estimate the diagnostic accuracy of the PTX detection
computer algorithm when compared to an expert panel of US trained physicians.
Methods: This was a retrospective study using archived thoracic US obtained on adult patients
presenting to the emergency department (ED) between 5/23/2011 and 8/6/2014. Emergency
medicine residents, fellows, attending physicians, physician assistants, and medical students
performed the US examinations and stored the images in the picture archive and communications
system (PACS). The PACS was queried for all ED bedside US examinations with reported positive
PTX during the study period along with a random sample of negatives. The computer algorithm then
interpreted the images, and we compared the results to an independent, blinded expert panel of
three physicians, each with experience reviewing over 10,000 US examinations.
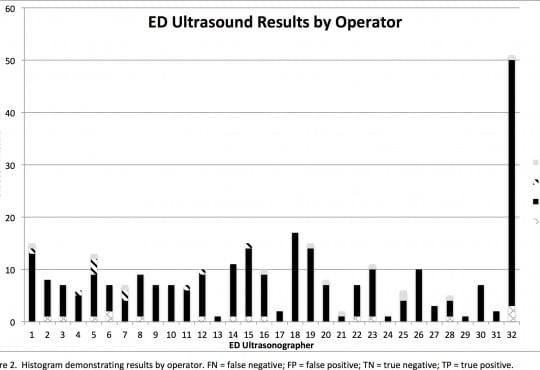
Results: Query of the PACS system revealed 146 bedside thoracic US examinations for analysis.
Thirteen examinations were indeterminate and were excluded. There were 79 true negatives, 33
true positives, 9 false negatives, and 12 false positives. The test characteristics of the algorithm
when compared to the expert panel were sensitivity 79% (95 % CI [63-89]) and specificity 87%
(95% CI [77-93]). For the 20 images scored as highest quality by the expert panel, the algorithm
demonstrated 100% sensitivity (95% CI [56-100]) and 92% specificity (95% CI [62-100]).
Conclusion: This novel computer algorithm has potential to aid clinicians with the identification of
the sonographic signs of PTX in the absence of expert physician sonographers. Further refinement
and training of the algorithm is still needed, along with prospective validation, before it can be utilized
in clinical practice.
Volume 17, Issue 2, March 2016.
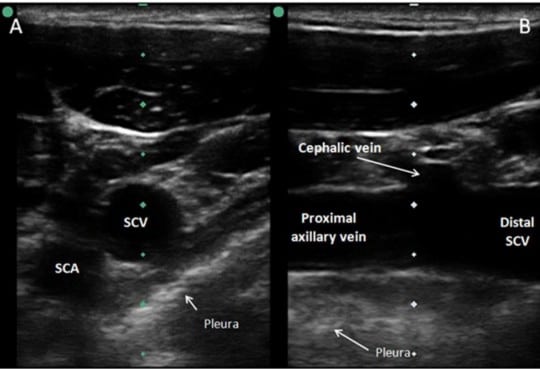
Talayeh Rezayat, DO, MPH, et al.
Despite multiple advantages, subclavian vein (SCV) cannulation via the traditional landmark
approach has become less used in comparison to ultrasound (US) guided internal jugular
catheterization due to a higher rate of mechanical complications. A growing body of evidence
indicates that SCV catheterization with real-time US guidance can be accomplished safely and
efficiently. While several cannulation approaches with real-time US guidance have been described,
available literature suggests that the infraclavicular, longitudinal “in-plane” technique may be
preferred. This approach allows for direct visualization of needle advancement, which reduces risk
of complications and improves successful placement. Infraclavicular SCV cannulation requires
simultaneous use of US during needle advancement, but for an inexperienced operator, it is more
easily learned compared to the traditional landmark approach. In this article, we review the evidence
supporting the use of US guidance for SCV catheterization and discuss technical aspects of the
procedure itself.
Volume 17, Issue 1, January 2015.
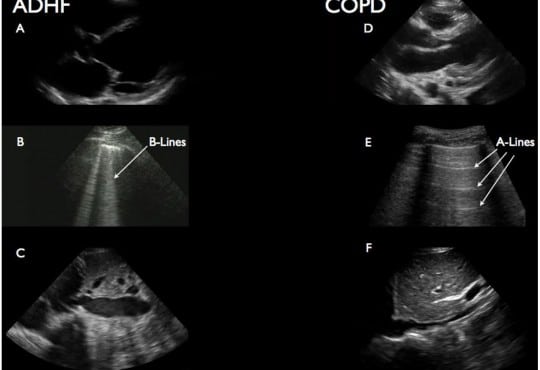
Daniel Mantuani, MD, et al.
Introduction: Determining the etiology of acute dyspnea in emregency department (ED) patients is
often difficult. Point-of-care ultrasound (POCUS) holds promise for improving immediate diagnostic
accuracy (after history and physical), thus improving use of focused therapies. We evaluate the impact
of a three-part POCUS exam, or “triple scan” (TS) – composed of abbreviated echocardiography,
lung ultrasound and inferior vena cava (IVC) collapsibility assessment – on the treating physician’s
immediate diagnostic impression.
Methods: A convenience sample of adults presenting to our urban academic ED with acute dyspnea
(Emergency Severity Index 1, 2) were prospectively enrolled when investigator sonographers
were available. The method for performing components of the TS has been previously described
in detail. Treating physicians rated the most likely diagnosis after history and physical but before
other studies (except electrocardiogram) returned. An investigator then performed TS and disclosed
the results, after which most likely diagnosis was reassessed. Final diagnosis (criterion standard)
was based on medical record review by expert emergency medicine faculty blinded to TS result.
We compared accuracy of pre-TS and post-TS impression (primary outcome) with McNemar’s
test. Test characteristics for treating physician impression were also calculated by dichotomizing
acute decompensated heart failure (ADHF), chronic obstructive pulmonary disease (COPD) and
pneumonia as present or absent.
Results: 57 patients were enrolled with the leading final diagnoses being ADHF (26%), COPD/
asthma (30%), and pneumonia (28%). Overall accuracy of the treating physician’s impression
increased from 53% before TS to 77% after TS (p=0.003). The post-TS impression was 100%
sensitive and 84% specific for ADHF.
Conclusion: In this small study, POCUS evaluation of the heart, lungs and IVC improved the
treating physician’s immediate overall diagnostic accuracy for ADHF, COPD/asthma and pneumonia
and was particularly useful to immediately exclude ADHF as the cause of acute dyspnea.
Volume 17, Issue 1, January 2016.
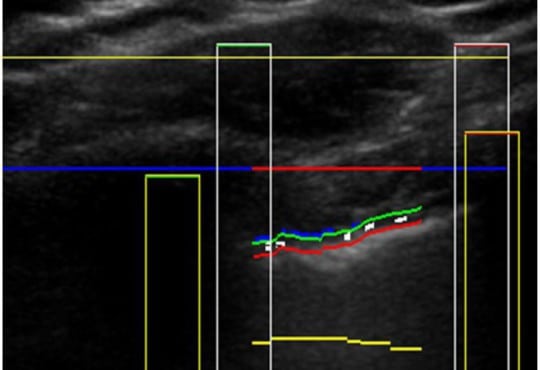
Mark Favot, MD, et al.
Echocardiography has become a critical tool in the evaluation of patients presenting to
the emergency department (ED) with acute cardiovascular diseases and undifferentiated
cardiopulmonary symptoms. New technological advances allow clinicians to accurately measure left
ventricular (LV) strain, a superior marker of LV systolic function compared to traditional measures
such as ejection fraction, but most emergency physicians (EPs) are unfamiliar with this method of
echocardiographic assessment.
This article discusses the application of LV longitudinal strain in the ED and reviews how it has been
used in various disease states including acute heart failure, acute coronary syndromes (ACS) and
pulmonary embolism.
It is important for EPs to understand the utility of technological and software advances in ultrasound
and how new methods can build on traditional two-dimensional and Doppler techniques of
standard echocardiography. The next step in competency development for EP-performed focused
echocardiography is to adopt novel approaches such as strain using speckle-tracking software in
the management of patients with acute cardiovascular disease. With the advent of speckle tracking,
strain image acquisition and interpretation has become semi-automated making it something
that could be routinely added to the sonographic evaluation of patients presenting to the ED with
cardiovascular disease. Once strain imaging is adopted by skilled EPs, focused echocardiography
can be expanded and more direct, phenotype-driven care may be achievable for ED patients with a
variety of conditions including heart failure, ACS and shock.
Volume 17, Issue 1, January 2016.
Adam Janicki, MD, et al.
A 64-year-old woman presented to the emergency department
after falling when she tripped on a rock while doing yard work.
Physical examination revealed an open deformity of the left
forearm (Figure 1). Radial pulse was palpable, sensation was
intact, and she had normal range of motion of the fingers. While
awaiting radiographs, bedside ultrasound was performed (Video).
Ultrasound revealed intact radius and ulna and a large linear
foreign body. The wooden foreign body was removed at the
bedside (Figure 2) and patient was admitted for observation and
intravenous antibiotics.
Volume 16, Issue 7, December 2015.
Bradley D. Gordon, MD, MS, et al.
Introduction: The objective of the study was to understand the immediate utility of health
information exchange (HIE) on emergency department (ED) providers by interviewing them shortly
after the information was retrieved. Prior studies of physician perceptions regarding HIE have only
been performed outside of the care environment.
Methods: Trained research assistants interviewed resident physicians, physician assistants and
attending physicians using a semi-structured questionnaire within two hours of making a HIE
request. The responses were recorded, then transcribed for qualitative analysis. The transcribed
interviews were analyzed for emerging qualitative themes.
Results: We analyzed 40 interviews obtained from 29 providers. Primary qualitative themes
discovered included the following: drivers for requests for outside information; the importance
of unexpected information; historical lab values as reference points; providing context when
determining whether to admit or discharge a patient; the importance of information in refining
disposition; improved confidence of provider; and changes in decisions for diagnostic imaging.
Conclusion: ED providers are driven to use HIE when they’re missing a known piece of information.
This study finds two additional impacts not previously reported. First, providers sometimes find
additional unanticipated useful information, supporting a workflow that lowers the threshold to
request external information. Second, providers sometimes report utility when no changes to their
existing plan are made as their confidence is increased based on external records. Our findings are
concordant with previous studies in finding exchanged information is useful to provide context for
interpreting lab results, making admission decisions, and prevents repeat diagnostic imaging.
Volume 16, Issue 7, December 2015.
Jestin N. Carlson, MD, MSc, et al.
Introduction: Video laryngoscopy (VL) has been advocated for several aspects of emergency
airway management; however, there are still concerns over its use in select patient populations
such as those with large volume hematemesis secondary to gastrointestinal (GI) bleeds. Given the
relatively infrequent nature of this disease process, we sought to compare intubation outcomes
between VL and traditional direct laryngoscopy (DL) in patients intubated with GI bleeding, using the
third iteration of the National Emergency Airway Registry (NEARIII).
Methods: We performed a retrospective analysis of a prospectively collected national database
(NEARIII) of intubations performed in United States emergency departments (EDs) from July 1, 2002,
through December 31, 2012. All cases where the indication for intubation was “GI bleed” were analyzed.
We included patient, provider and intubation characteristics. We compared data between intubation
attempts initiated as DL and VL using parametric and non-parametric tests when appropriate.
Results: We identified 325 intubations, 295 DL and 30 VL. DL and VL cases were similar in terms
of age, sex, weight, difficult airway predictors, operator specialty (emergency medicine, anesthesia
or other) and level of operator training (post-graduate year 1, 2, etc). Proportion of successful first
attempts (DL 261/295 (88.5%) vs. VL 28/30 (93.3%) p=0.58) and Cormack-Lehane grade views
(p=0.89) were similar between devices. The need for device change was similar between DL [2/295
(0.7%) and VL 1/30 (3.3%); p=0.15].
Conclusion: In this national registry of intubations performed in the ED for patients with GI bleeds,
both DL and VL had similar rates of success, glottic views and need to change devices.
Volume 16, Issue 7, December 2015.
Shadi Lahham, MD, MS, et al.
A 61-year-old female was brought in by ambulance after
being the restrained driver of a head-on motor vehicle collision
at 40MPH. There was positive airbag deployment and intrusion
from the other vehicle. During workup, the patient complained
of midline chest pain, and left chest wall pain. The patient
was not in acute respiratory distress, and had the following
vital signs: temperature 37°C, heart rate 84, blood pressure
of 150/64, respiratory rate 18, and oxygen saturation of 97%
on two liters of oxygen. On physical exam, breath sounds
were heard bilaterally, with no acute cardiopulmonary issues
identified. A bruise was identified on the lower abdomen,
which was thought to be a potential seatbelt sign. A focused
assessment with sonography for trauma was negative, and an
ultrasound of additional chest and mediastinal structures was
performed for the chest tenderness.
Volume 16, Issue 5, September 2015.
Jason L. Sanders, MD, PhD, et al.
Introduction: Growing evidence supports emergency physician (EP)-performed point-of-care
ultrasound (PoC US). However, there is a utilization gap between academic emergency departments
(ED) and other emergency settings. We elucidated barriers to PoC US use in a multistate sample
of predominantly non-academic EDs to inform future strategies to increase PoC US utilization,
particularly in non-academic centers.
Methods: In 2010, we surveyed ED directors in five states (Arkansas, Hawaii, Minnesota,
Vermont, and Wyoming; n=242 EDs) about general ED characteristics. In four states we
determined barriers to PoC US use, proportion of EPs using PoC US, use privileges, and
whether EPs can bill for PoC US.
Results: Response rates were >80% in each state. Overall, 47% of EDs reported PoC US
availability. Availability varied by state, from 34% of EDs in Arkansas to 85% in Vermont. Availability
was associated with higher ED visit volume, and percent of EPs who were board certified/board
eligible in emergency medicine. The greatest barriers to use were limited training (70%), expense
(39%), and limited need (perceived or real) (32%). When PoC US was used by EPs, 50% used it
daily, 44% had privileges not requiring radiology confirmation, and 34% could bill separately for PoC
US. Only 12% of EPs used it ≥80% of the time when placing central venous lines.
Conclusion: Only 47% of EDs in our five-state sample of predominantly non-academic EDs had
PoC US immediately available. When available, the greatest barriers to use were limited training,
expense, and limited need. Recent educational and technical advancements may help overcome
these barriers.
Volume 16, Issue 5, September 2015.
Thompson Kehri, MD, et al.
Cardiac arrest in the adolescent population secondary to congenital heart disease (CHD) is rare.
Focused cardiac ultrasound (FoCUS) in the emergency department (ED) can yield important clinical
information, aid in resuscitative efforts during cardiac arrest and is commonly integrated into the
evaluation of patients with pulseless electrical activity (PEA). We report a case of pediatric cardiac
arrest in which FoCUS was used to diagnose a critical CHD known as cor triatriatum sinistrum
as the likely cause for PEA cardiac arrest and help direct ED resuscitation.
Volume 16, Issue 5, September 2015.
Thomas M. Nappe, Do, et al.
A 56-year-old female presented to the emergency
department (ED) with a chief complaint of urinary retention
and overflow incontinence for 24 hours, preceded by
progressive difficulty with voiding, worsening lower
abdominal discomfort and bloating. Her past medical
history was significant for small bowel obstruction and
neurofibromatosis with an associated benign pelvic tumor that
caused similar symptoms as a child, but had been known to
be stable since that time. She had also recently been treated
for a urinary tract infection. Her physical exam revealed
tachycardia and a diffusely tender abdomen with a palpable,
tender suprapubic mass extending just above her umbilicus.
Volume 16, Issue 5, September 2015.
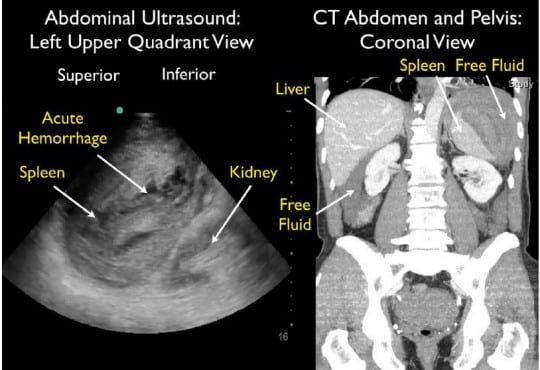
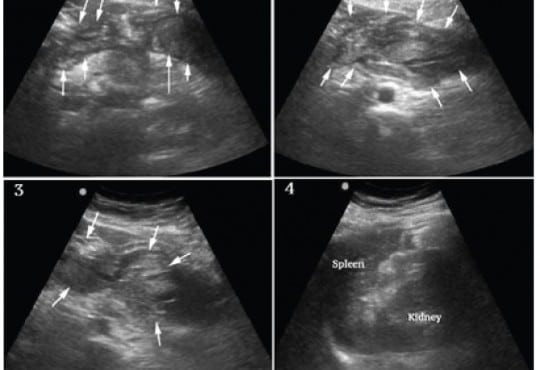
William Mulkerin, MD, et al.
A 64-year-old male presented to the emergency
department (ED) with near syncope and worsening left flank
and shoulder pain. He had undergone a difficult colonoscopy
two days prior due to a tortuous colon. Initial vital signs
were normal. He looked uncomfortable and had significant
left upper quadrant abdominal tenderness with guarding.
Thirty minutes after ED arrival, his blood pressure dropped
to 73/59 mmHg, requiring aggressive fluid resuscitation.
Bedside focused assessment with sonography in trauma
(FAST) exam demonstrated free fluid in the abdomen with
mixed echogenicity of the spleen, suggestive of splenic injury.
Computed tomography (CT) demonstrated a large subcapsular
splenic hematoma with active extravasation and surrounding
intraperitoneal free fluid.
Volume 16, Issue 5, September 2015.
Jason D. Heiner, MD
A 72-year-old otherwise healthy female presented to
the emergency department with two weeks of worsening
abdominal pain. She was afebrile with normal vital signs. Her
physical examination was notable for moderate abdominal
tenderness without rebound to the left and suprapubic
regions of the abdomen. Laboratory studies were remarkable
for a white blood cell count of 13,000/mm3
. A focused
bedside ultrasound over the patient’s region of maximal
discomfort revealed a thickened bowel wall and several
small contiguous hypoechoic projections surrounding a
hyperechoic center, suggestive of diverticulitis.
Volume 16, Issue 5, September 2015.
Terri Davis, MSHS, PA-C, et al.
Splenic artery aneurysm rupture is rare and potentially fatal. It has largely been reported in pregnant
patients and typically not diagnosed until laparotomy. This case reports a constellation of clinical and
sonographic findings that may lead clinicians to rapidly diagnose ruptured splenic artery aneurysm
at the bedside. We also propose a rapid, but systematic sonographic approach to patients with
atraumatic hemoperitoneum causing shock. It is yet another demonstration of the utility of bedside
ultrasound in critically ill patients, specifically with undifferentiated shock.
Volume 16, Issue 4, July 2015.
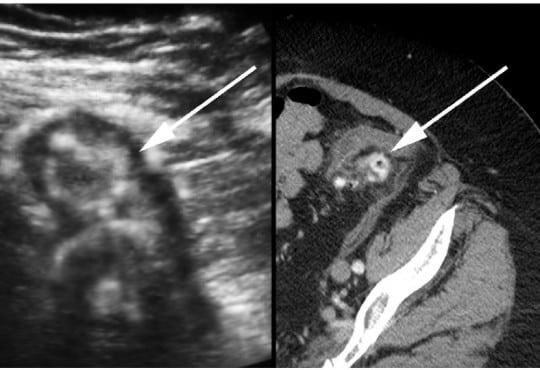
Subramony, MD, et al.
Choledochal cysts are rare but serious bile duct abnormalities are found in young children, usually during the first year of life. They require urgent surgical intervention due to the risk of developing cholangiocarcinoma. Clinicians should consider this diagnosis and perform a point-of-care ultrasound (POCUS) when a child presents to the emergency department (ED) with findings of jaundice, abdominal pain, and the presence of an abdominal mass. We present the case of a six-year-old child presenting only with abdominal pain upon arrival to our ED and was ultimately diagnosed by POCUS to have a choledochal cyst.
{kind=link}