
{kind=link}
| Author | Affiliation |
|---|---|
| Brad E. Talley, MD | Denver Health Medical Center |
| Adit A. Ginde, MD, MPH | University of Colorado School of Medicine |
| Ali S. Raja, MD, MBA | Brigham and Women’s Hospital |
| Ashley F. Sullivan, MS, MPH | Massachusetts General Hospital, Harvard Medical School |
| Janice A. Espinola, MPH | Massachusetts General Hospital, Harvard Medical School |
| Carlos A. Camargo, Jr., MD, DrPH | Massachusetts General Hospital, Harvard Medical School |
ABSTRACT
Introduction:
Use of bedside emergency department (ED) ultrasound has become increasingly important for the clinical practice of emergency medicine (EM). We sought to evaluate differences in the availability of immediate bedside ultrasound based on basic ED characteristics and physician staffing.
Methods:
We surveyed ED directors in all 351 EDs in Colorado, Georgia, Massachusetts, and Oregon between January and April 2009. We assessed access to bedside ED ultrasound by the question: “Is bedside ultrasound available immediately in the ED?” ED characteristics included location, visit volume, admission rate, percent uninsured, total emergency physician full-time equivalents and proportion of EM board-certified (BC) or EM board-eligible (BE) physicians. Data analysis used chi-square tests and multivariable logistical regression to compare differences in access to bedside ED ultrasound by ED characteristics and staffing.
Results:
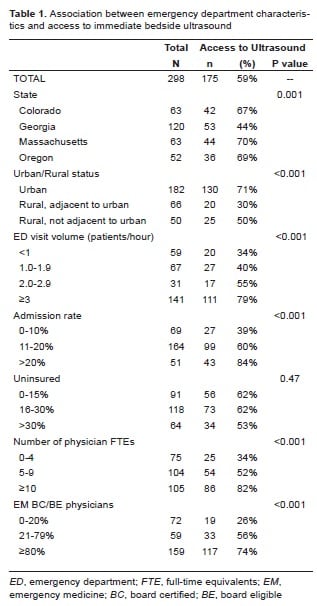
We received complete responses from 298 (85%) EDs. Immediate access to bedside ultrasound was available in 175 (59%) EDs. ED characteristics associated with access to bedside ultrasound were: location (39% for rural vs. 71% for urban, P<0.001); visit volume (34% for EDs with low volume [<1 patient/hour] vs. 79% for EDs with high volume [≥3 patients/hour], P<0.001); admission rate (39% for EDs with low [0–10%] admission rates vs. 84% for EDs with high [>20%] rates, P<0.001); and EM BC/BE physicians (26% for EDs with a low percentage [0–20%] vs.74% for EDs with a high percentage [≥80%], P<0.001).
Conclusion:
U.S. EDs differ significantly in their access to immediate bedside ultrasound. Smaller, rural EDs and those staffed by fewer EM BC/BE physicians more frequently lacked access to immediate bedside ultrasound in the ED.
INTRODUCTION
Bedside ultrasonography has become an integral part of emergency department (ED) care and an increasingly important tool for emergency physicians. It provides rapid, real time information that assists in patient care and clinical decision-making.1–4 Because of its demonstrated value, ED ultrasound has been integrated into emergency medicine (EM) residency training and has become a standard skill set provided by emergency physicians.5
Favorable assessments of bedside ED ultrasound come primarily from large, urban, academic centers where training and access to ultrasound is readily available.13 However, these institutions comprise only a minority of United States (U.S.) EDs, to which most of the U.S. population has limited access.6,7 Little is known about the use of ED ultrasound outside these urban, academic hospitals. Two prior studies investigating ultrasound use in the community setting have shown decreased use of ED ultrasound compared to the academic setting, but neither of these studies looked specifically at the effect of rural location on ED ultrasound use.11,12 Further understanding of ED ultrasound use in the general community, particularly in small, rural EDs, would help educators to target ultrasound training and outreach, as well as improve access to high quality emergency care in all EDs.
In this study, we sought to evaluate overall access to immediate bedside ED ultrasound and differences in access based on basic ED characteristics and physician staffing. We hypothesized that small, rural EDs and those with fewer EM board-certified (BC) or board-eligible (BE) physicians would have less access to bedside ED ultrasound.
METHODS
We conducted a survey of physician or nurse directors of all 351 EDs in Colorado, Georgia, Massachusetts and Oregon between January and April of 2009. Each state investigator’s Institutional Review Board approved the study with a waiver of written informed consent.
We used the 2007 version of the National Emergency Department Inventories (NEDI)-USA database to obtain a comprehensive list of all nonfederal U.S. hospitals with EDs in the four included states (n=351). Methods for derivation of NEDI-USA have been previously described.6 Briefly, NEDI-USA combines data from three sources: Verispan Marketing Group’s Hospital Market Profiling Solution Database (Yardley, PA), the American Hospital Association Annual Survey of the Hospitals (Chicago, IL), and information collected independently by Emergency Medicine Network (Boston, MA) staff. EDs were defined as emergency care facilities open 24 hours per day, seven days per week and available for use by the general public. We excluded federal hospitals (e.g. Veterans Affairs and Indian Health Service hospitals), military hospitals and college infirmaries as these are not available through NEDI-USA.
We mailed the survey to ED directors three times over a two-month period. We contacted non-responders and those with partial or incomplete responses by telephone for completion. The survey assessed access to bedside ED ultrasound by the following question: “Is bedside ultrasound available immediately in the ED?”
We classified ED location as urban and rural (adjacent to urban or not adjacent to urban) using the county-based 2003 urban influence codes (www.usda.gov). Other ED characteristics included in the survey were number of ED patients seen per hour (calculated from annual visit volume), and hospital admission rate. Physician staffing characteristics included total emergency physician full-time equivalents and proportion of EM BC/BE physicians by the American Board of Emergency Medicine, American Osteopathic Board of Emergency Medicine, or the American Board of Pediatrics (Pediatric EM).
Data Analysis
We performed statistical analyses using Stata 10.1 (StataCorp, College Station, TX) and summarized data using basic descriptive statistics. We performed the univariable analyses using chi-square tests to compare differences in access to bedside ED ultrasound by ED characteristics and physician staffing. All p values were two-tailed, with p<0.05 considered statistically significant. We then performed multivariable logistical regression to evaluate independent predictors of access to ED bedside ultrasound with results reported as odds ratios (ORs) with 95% confidence intervals (CIs). We included all ED characteristics obtained from the survey, regardless of significance in univariable testing, in the multivariable model.
RESULTS
We obtained complete responses from 298 (85%) of the 351 EDs in the four participating states. The missing 15% was the result of not receiving a completed survey or from not having phone calls returned or answered from ED directors. Overall, 175 (59%; 95%CI, 53–64) had immediate access to bedside ED ultrasound. The tables show access to ultrasound by ED characteristics and physician staffing.
Massachusetts had the highest bedside ED ultrasound access, while Georgia had the lowest. ED characteristics associated with less access to bedside ED ultrasound were: rural location, lower visit volume and lower admission rate. ED physician staffing associated with less access to bedside ED ultrasound were: lower emergency physician full-time equivalents and lower percentage of EM BC/BE physicians.
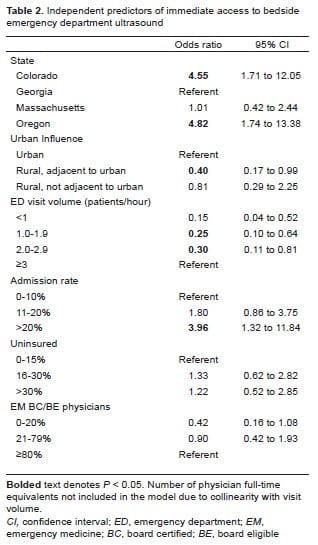
In the multivariable logistic regression, independent predictors of access to bedside ED ultrasound were ED location, visit volume and admission rate. Rural (adjacent to urban) EDs had less access to ultrasound (OR 0.40 [95%CI, 0.17–0.99]) than urban EDs. Compared to EDs with ≥3 patients per hour, EDs with lower visit volumes had less access to ultrasound (OR 0.15 [95%CI, 0.04–0.52] for <1 patient per hour; OR 0.25 [95%CI, 0.10–0.64] for 1–1.9 patients per hour; and OR 0.30 [95%CI, 0.11–0.81] for 2.0–2.9 patients per hour). Additionally, EDs with admission rates >20% had more access to ultrasound (OR 3.96 [95%CI, 1.32–11.84]) than those with admission rates of ≤10%. After adjusting for ED characteristics, physician staffing was not independently associated with access to bedside ED ultrasound.
DISCUSSION
In a four-state study, with 85% participation, we found that immediate access to bedside ED ultrasound was available in only 59% of EDs. Availability varied significantly by state and by ED characteristics; smaller, rural EDs and those with lower admission rates had significantly less access to bedside ED ultrasound. EDs staffed with a smaller percentage of EM BC/BE physicians had less access to bedside ED ultrasound, although confounding by ED location and visit volume appeared to account for this difference.
These findings have important implications for access to high-quality emergency care and patient safety, especially in smaller, rural EDs. The value of bedside ED ultrasound has been well established in the literature, particularly in situations that require immediate medical decisions and rapid interventions that cannot afford the delay caused by waiting for radiology to perform and interpret an ultrasound study. Specifically, ED ultrasound improves patient safety by decreasing the risks associated with obtaining central venous access, as well as by obviating invasive procedures such as peritoneal lavage, culdocentesis and blind pericardiocentesis.1,2 Having immediate access to an ED ultrasound machine and appropriately trained providers also improves ED efficiency by providing real-time images without the delay of ordering, performing, and interpreting radiology-performed sonographic studies, which may not be readily available. This efficiency can decrease ED length of stay, help alleviate ED crowding, and most importantly improve emergency care for the patient.3–4
While ED characteristics, rather than physician staffing, were most predictive of access to bedside ED ultrasound, our study could not specifically address the reason for these differences. Smaller, rural EDs may not have the patient volume or acuity to financially justify owning a bedside ED ultrasound. Additionally, many smaller, rural EDs are staffed by midlevel providers and non-EM BC/BE physicians.8–9 These providers may not be trained to perform and interpret ultrasound studies, limiting the use of bedside ED ultrasound in their practice. Prior studies have demonstrated a shortage of EM BC/BE physicians,9 which will likely continue for several decades.10
Many healthcare providers staffing smaller, rural EDs may not be trained in the use of ultrasound and therefore may not use it to enhance emergency care. Our study suggested that EDs staffed with fewer EM BC/BE physicians had less access to bedside ultrasound. Education and outreach to these small, rural EDs may improve ultrasound training and result in greater access to ultrasound for those patients. Further study is needed to evaluate if increased training and access to bedside ED ultrasound results in a measureable change in quality of emergency care and cost-effectiveness of beside ultrasound for these EDs. While bedside ED ultrasound represents only one important component of ED care, it represents a gap in the ability to provide high-quality emergency care in rural EDs.
LIMITATIONS
The study has several potential limitations. Although we obtained a >80% response rate from all of the EDs in each state, response bias may have affected our results. Specifically, nonresponding EDs may be more likely to have less access to bedside ED ultrasound. However, the urban-rural status and ED visit volumes of nonresponding EDs were similar to those that did respond (data not shown). Additionally, our survey data were limited by reliance on self-reporting. However, ED directors, who were knowledgeable about their ED characteristics and capabilities, were surveyed. However, since survey responses were anonymous, we cannot know if the ED director completed the survey alone or required assistance. Finally, the survey used a single question to evaluate access to bedside ED ultrasound and did not ask about reasons for lack of access nor its actual use. We assumed that immediate access to bedside ED ultrasound was a valid marker for use by ED providers. However, the availability of immediate bedside ultrasound does not require that the ultrasound be performed by the emergency physician; it is possible that a technician or a radiologist could still perform the study. We plan to build on the present results with additional ultrasound-focused questions in future studies to address some of these limitations.
CONCLUSION
There are significant differences in access to bedside ED ultrasound based on ED characteristics and physician staffing. Smaller, rural EDs and those staffed by fewer EM BC/BE physicians had less access to bedside ED ultrasound. Given the proven use of bedside ultrasound in the evaluation and treatment of ED patients, observed differences in access should encourage EM educators and administrators to focus on the diffusion of bedside ultrasound training and access in both small and rural EDs.
Footnotes
Supervising Section Editor: J Christian Fox, MD
Submission history: Submitted January 23, 2010; Revision received May 18, 2010; Accepted July 6, 2010.
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Carlos A. Camargo, MD, DrPH, Department of Emergency Medicine, Massachusetts General Hospital, 326 Cambridge St. Suite 410, Boston, MA 02114
Email: ccamargo@partners.org
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Leung J, Duffy M, Finckh A. Real-time ultrasonographically-guided internal jugular vein catheterization in the emergency department increases success rates and reduces complications: a randomized, prospective study. Ann Emerg Med. 2006;5:540–7. [PubMed]
2. Ollerton JE, Sugrue M, Balogh Z, et al. Prospective study to evaluate the influence of FAST on trauma patient management. J Trauma. 2006;4:785–91. [PubMed]
3. Shih CH. Effect of emergency physician-performed pelvic sonography on length of stay in the emergency department. Ann Emerg Med. 1997;29:348–51. [PubMed]
4. Blaivas M, Harwood RA, Lambert MJ. Decreasing length of stay with emergency ultrasound examination of the gallbladder. Acad Emerg Med. 1999;6:1020–3. [PubMed]
5. Heller MB, Mandavia D, Tayal VS, et al. Residency training in emergency ultrasound: fulfilling the mandate. Acad Emerg Med. 2002;9:835–9. [PubMed]
6. Sullivan AF, Richman IB, Ahn CJ, et al. A profile of US emergency departments in 2001. Ann Emerg Med. 2006;48:694–701. [PubMed]
7. Carr BG, Branas CC, Metlay JP, et al. Access to emergency care in the United States. Ann Emerg Med. 2009;54:261–71. [PMC free article] [PubMed]
8. Ginde AA, Espinola JA, Sullivan AF, et al. Use of physician assistants and nurse practitioners in United States emergency departments, 1993–2005: implications for the emergency physician workforce. Am J Emerg Med. 2009 in press.
9. Ginde AA, Sullivan AF, Camargo CA., Jr National study of the emergency physician workforce 2008. Ann Emerg Med. 2009;54:349–59. [PubMed]
10. Camargo CA, Jr, Ginde AA, Singer AH, et al. Assessment of emergency physician workforce needs in the United States, 2005. Acad Emerg Med. 2008;15:1317–20. [PubMed]
11. Moore CL, Molina AA, Lin H. Ultrasonography in community emergency departments in the United States: access to ultrasonography perfomed by consultants and status of emergency physician-performed ultrasonography. Ann Emerg Med. 2006;47:147–53. [PubMed]
12. Stein JC, River G, Kalika I, et al. A survey of bedside ultrasound use by emergency physicians in California. J Ultrasound Med. 2009;28:757–63. [PubMed]
13. American College of Emergency Physicians Use of ultrasound imaging by emergency physicians [policy #40121] Ann Emerg Med. 2001;38:469–70. [PubMed]