
{kind=link}
| Author | Affiliation |
|---|---|
| Julie Gorchynski, MD, MSc | JPS Health Network, Fort Worth, Department of Emergency Medicine, University of Texas, Southwestern |
| Kevin Dean, MD | Oregon Adventist, Department of Emergency Medicine |
| Craig L. Anderson, PhD, MPH | University of California, Irvine School of Medicine |
ABSTRACT
Introduction:
To determine the point prevalence of urine bilirubin, urine hemoglobin and urobilinogen in blunt trauma patients, and to evaluate its utility as a screening tool for intra-abdominal injury.
Methods:
Data analysis of 986 consecutive trauma patients of which 698 were adult blunt trauma patients. Five-hundred sixteen subjects had a urinalysis and a CT scan of the abdomen/pelvis or exploratory laparotomy. We reviewed initial urinalysis results from trauma patients in the emergency department (ED) for the presence of urine hemoglobin, uroblinogen and urine bilirubin. Computed tomography (CT) scan results and operative reports were reviewed from the trauma registry for evidence of liver laceration, spleen laceration, bowel or mesenteric injuries.
Results:
There were 73 injuries and 57/516 patients (11%) with intra-abdominal injury. Urinalysis was positive for urobilinogen in 28/516 (5.4%) patients, urine bilirubin in 15/516 (2.9%) patients and urine hemoglobin in 313/516 (61%) patients. Nineteen/forty-seven (4%) subjects had liver lacerations, 28/56 (5%) splenic lacerations, and 15/5 (3%) bowel or mesenteric injury. Comparing the proportion of patients that had urobilinogen detected in the group with and without intra-abdominal injury, 8/28 (29%) subjects with urobilinogen, 5/15 (33%) subjects with bilirubin and 47/313 (15%) subjects with urine hemoglobin were found to have liver lacerations, spleen lacerations, or bowel/mesenteric injuries. Preexisting liver or biliary conditions were not statistically associated with elevation of urine bilirubin, urine hemoglobin or urobilinogen on initial urinalysis after blunt abdominal trauma. Point prevalence for urobilinogen, urine bilirubin and urine hemoglobin are 5.43% (28/516), 2.91% (15/516) and 60.7% (313/516) respectively.
Conclusion:
The utility of the initial routine urinalysis in the ED for adult blunt abdominal trauma patients should not be used as a screening tool for the evaluation of intra-abdominal injury.
INTRODUCTION
Multiple studies in the emergency medicine (EM) and pathology literature in the late 1980s showed a quantitative correlation between urobilinogen and serum liver enzymes [aspartate aminotransferase (AST) and alanine aminotransferase (ALT)] that demonstrated urobiliogen as a useful screening marker of liver dysfunction in non-trauma medical patients presenting to the emergency department (ED).1,2 The presence of urine bilirubin is described as highly specific for elevated serum bilirubin due to hepatocellular or biliary tree injury, rather than intravascular hemolysis.1,2 It follows that there may be a similar association in trauma patients as a screening tool for liver injury after blunt abdominal trauma. The value of routine screening laboratory tests in trauma patients has been debated repeatedly in the literature.3,4 Many studies have attempted to establish an association between abnormal lab test results and occult injury as a way to target imaging studies more effectively.5,6,7 In 2002 Holmes et al.4demonstrated an association between elevated serum aminotransferases and liver injury in pediatric trauma patients.4 Conversely, in a study conducted in 2004 Keller et al.3refuted the association reported by Holmes, thereby casting doubt on the predictive value of routine organ-specific laboratory studies in trauma patients.3 The urinalysis (UA) is routinely obtained on all trauma victims who present to the ED primarily as a screening tool for renal or bladder injury. Apart from the red blood cell counts, the remainder of the UA is not routinely used as markers of potential solid or hollow organ injury. The utility of urobilinogen and urine bilirubin in blunt abdominal trauma has not been studied in a systematic fashion.
The objective of this study was to determine the point prevalence of urobilinogen, urine bilirubin and urine hemoglobin in adult blunt abdominal trauma patients with liver, spleen, bowel or mesenteric injuries. The secondary outcome was to evaluate the utility of the routine UA in blunt trauma patients as a screening tool for intra-abdominal injury.
METHODS
A cross-sectional study was conducted on consecutive patients with blunt abdominal trauma that presented to a university tertiary care Level I trauma center with an annual census of 50,000. All patients were identified from the existing trauma registry. Inclusion criteria included all blunt abdominal trauma patients, ≥18 years who presented to the ED and required trauma team activation. This was determined by mechanism of injury, vital signs and Glascow Coma Scale score. In addition, subjects must have received an initial UA in the ED and a CT scan of the abdomen/pelvis or exploratory laparotomy. Subjects excluded were patients less than 18 years old, penetrating trauma patients, anuric (i.e. dialysis-dependent) patients, and those subjects that did not receive a CT scan of the abdomen/pelvis or exploratory lapartomy.
We identified the study cohort through the existing trauma database and obtained basic demographic data on each patient. From this database we determined the types of radiographic studies and lab tests performed and obtained the operative reports. Patient medical record numbers were used to link specific radiographic and laboratory results for subjects of interest and abstracted from existing electronic patient medical records onto a data collection instrument. The individual patients were not contacted, and there was no patient follow up data available after the initial trauma evaluation. We reviewed UA results for the presence of urine hemoglobin, urobilinogen and urine bilirubin, and also collected data on urine specific gravity, pH, red blood cells, white blood cells, and protein (“0” to “500 mg/dL”). After CT scan results were obtained from dictated radiology reports and operative findings from operative reports, we reviewed them for evidence of liver or spleen lacerations, and bowel or mesenteric injury. Patient medical history was obtained from dictated “trauma run” reports, and were based on information gathered from patients, family members, and Emergency Medical Services (EMS) personnel. We also reviewed patient medical records for history of preexisting hepatobiliary pathology.
The study was approved by the hospital institutional review board. We used standard measures of diagnostic accuracy using the Stata program (version 10, College Station, TX).8
RESULTS
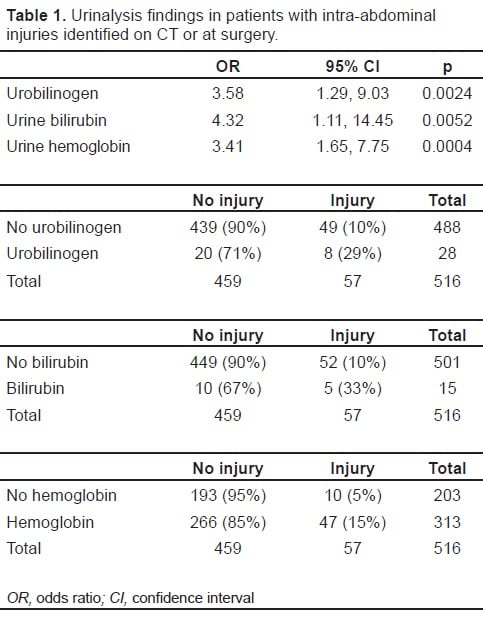
We reviewed 986 consecutive trauma patients’ medical data and identified 698 (71%) blunt abdominal trauma subjects. From this database 516/986 (52%) subjects met inclusion criteria: 343 (66%) males and 173 (34%) females. Subjects were 18–99 years (mean = 58). There were 291 motor vehicle collisions (56.4%), 65 falls (12.6%), 55 automobile vs. pedestrian accidents (10.7%), 38 motorcycle accidents (7.4%), 37 assaults (7.2%), four crush injuries (0.8%), two quadruped accidents (0.4%) and one sports injury (0.2%). There were 57 patients (11.1% of 516 study patients) with 73 different intra-abdominal injuries. Forty-three subjects had documented hepatobiliary disease, which consisted of one subject with Hepatitis B and four with Hepatitis C, while eight had a prior cholecystectomy and 16 had incidental findings of cholelithiasis. Past medical history was unknown in 433(84%) subjects. UA was positive for urobilinogen in 28 (5.4%) subjects, urine bilirubin in 15 (2.9%), and urine hemoglobin in 313 (61%). There were 19 (3.7 %) liver lacerations, 28 (5.4%) splenic lacerations, and 15 (2.9%) bowel or mesenteric injury. Eight of 28 (29%) subjects with urobilinogen, five of 15 (33%) with urine bilirubin and 47 of 313 (15 %) with urine hemoglobin had blunt abdominal injury with documented liver or spleen lacerations, or bowel injuries (Table 1).
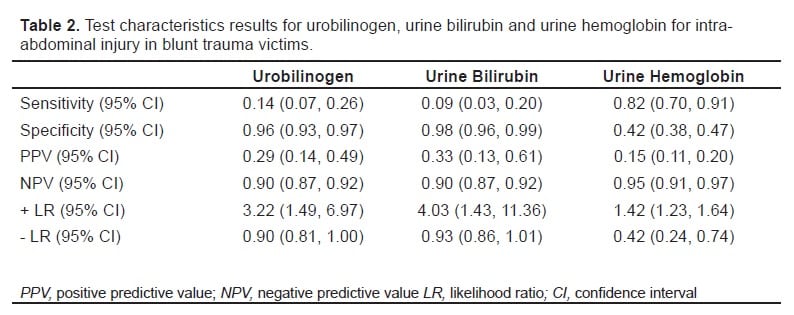
The presence of urobilinogen, urine bilirubin and urine hemoglobin on initial UA after blunt abdominal trauma appears to be a predictor of intra-abdominal injury. See Table 2for sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (+LR) and negative likelihood ratio (−LR) and associated confidence intervals (CI).
DISCUSSION
Urinalysis has long been considered an essential part of standard trauma adjunctive testing for possible renal or bladder injury. This is the first study to examine the utility of UA with the presence of urobilinogen, urine bilirubin and urine hemoglobin as an indicator in the acute evaluation of blunt abdominal trauma patients for intra-abdominal injury. It demonstrates a statistically significant association between the presence of urine bilirubin, urobilinogen, and urine hemoglobin and intra-abdominal injury. However, the utility of routine UA of the blunt abdominal trauma patient as a predictor of intra-abdominal injury is not strong enough to be clinically useful. The sensitivities and PPV for urobilinogen and urine bilirubin are low, while the specificity and NPV are high. These high specificities and NPVs are deceptive as they are a consequence of low prevalence of injury in the sample population and are accompanied by poor sensitivity with many false negative test results. The converse is true for urine hemoglobin, which is a non-specific indicator of injury with many false positive results.
The utility of the initial routine UA in the ED for adult blunt abdominal trauma patients is a poor predictor for intra-abdominal injury. The LRs found here are not sufficient to change patient management in a resource-rich environment. However, under austere conditions where CT imaging or surgery is less available, these findings, if possible, might be useful to increase suspicion of injury.
LIMITATIONS
This retrospective study from a trauma patient registry data suffers from incomplete information on past medical history, as injured patients are unable to provide medical history and are often not accompanied by family members. This registry data was not supplemented by patient follow up. We had a small number of patients with documented injuries from which to draw conclusions. Additionally, blunt abdominal trauma patients may suffer from hypovolemic shock, which may have reduced renal perfusion and thus urine output leading to false negative results.2 Furthermore, we did not assess the effects of prerenal azotemia and metabolic acidosis on the metabolism of bilirubin and urobilinogen. Finally, short EMS transport times and rapid initial trauma assessment, with urine taken immediately on ED presentation, may have led to samples being obtained before bilirubin breakdown products were present in urine in sufficient quantities for detection.
CONCLUSION
The presence of urobilinogen, urine bilirubin or urine hemoglobin in the initial routine UA in the adult blunt abdominal trauma patient, although statistically associated with intra-abdominal injury, is not a useful clinical adjunct to standard evaluation.
Footnotes
Supervising Section Editor: Tareg Bey, MD
Submission history: Submitted August 09, 2007; Revision Received November 08, 2008; Accepted December 03, 2008
Full text available through open access at http://escholarship.org/uc/uciem_westjem
Address for Correspondence: Julie Gorchynski, MD, MSc. JPS Health Network, Medical Director, Department of Emergency Medicine, Director of Research, 1500 South Main St., Fort Worth, TX 76104
Email: jgorchyn@msn.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Brenner B, Rector F. Brenner & Rector’s The Kidney. 7th edition. Philadelphia, PA: Sanders Publication; 2004. pp. 1121–1123.
2. Chowdhury J, Chowdhury N. Conjugation and excretion of bilirubin. Seminars in Liver Disease. 1983;3:11–23. [PubMed]
3. Keller MS, Coln CE, Trimble JA, Green MC, Weber TR. The utility of routine trauma laboratories in pediatric trauma resuscitations. Am J Surg. 2004;188:671–678.[PubMed]
4. Holmes JF, Sokolove P, Brant W. Identification of children with intra-abdominal injuries after blunt trauma. Ann Emerg Med. 2002;39:500–509. [PubMed]
5. Cotton BA, Beckert B, Smith M. The utility of clinical and laboratory data for predicting intraabdominal injury among children. J Trauma. 2004;56:1068–1075. [PubMed]
6. Holmes JF, Sokolove P, Land C. Identification of intra-abdominal injuries in children hospitalized following blunt torso trauma. Acad Emerg Med. 1999;6:799–806. [PubMed]
7. Puranik SR, Hayes J, Long J. Liver Enzymes as predictors of liver damage due to blunt abdominal trauma in children. South Med J. 2002;95:203–206. [PubMed]
8. Newcombe RG. Two-sided confidence intervals for the single proportion: comparison of seven methods. Stat Med. 1998;17:857–872. [PubMed]