
{kind=link}
| Author | Affiliation |
|---|---|
| David Bell, MD, PhD | Maricopa Medical Center, Department of Emergency Medicine, Phoenix, Arizona |
| Eric Katz, MD | Maricopa Medical Center, Department of Emergency Medicine, Phoenix, Arizona |
| Anne Klokow, MD | Maricopa Medical Center, Department of Emergency Medicine, Phoenix, Arizona |
Introduction
Case report
Discussion
Conclusion
ABSTRACT
This case report details the emergency department course of a 34 year-old female who presented with abdominal pain and vaginal bleeding after reportedly falling one week earlier. She was subsequently found to have a drinking straw within her uterus next to an eight week-old live intrauterine pregnancy on ultrasound. This case report and discussion reviews the literature on retained foreign bodies in pregnancy while addressing the added complications of an evasive patient and a difficult consultant with significant intra-specialty disagreement.
INTRODUCTION
In many ways, the medicine we practice as emergency physicians (EPs) is straightforward. Part of the rewarding nature of our field is simply due to that simplicity—a patient comes in with an acute problem, we hopefully resolve the problem, and the patient leaves satisfied while we receive high Press-Ganey scores. And yet sometimes, we stumble across cases that challenge us both ethically and intellectually. This is one such case. A difficult patient, an unusual medical problem, and an obstinate consultant all come together to highlight several unique challenges that we commonly encounter in emergency medicine, but which we rarely consider at length.
CASE REPORT
The patient was a 34-year-old female with a chief complaint of abdominal pain. Her triage vitals were blood pressure 110/57; heart rate 93; respiratory rate 16; temperature 36.4°C. She stated she fell in her yard several days ago resulting in abdominal pain with some vaginal bleeding starting the morning of presentation. Upon further discussion during the physical exam, the patient admitted she missed her period and, in an effort to initiate it, stuck a drinking straw into her vagina. She inserted the whole straw inside and could still feel it poking her. She denied being pregnant and insisted she simply wanted to begin her period. Her pelvic exam was benign with a closed os, minimal blood in the vault, minimal right adnexal tenderness, and no signs of a foreign body or any lacerations. Basic labs revealed the patient was pregnant with a βHCG of 90,034. A subsequent ultrasound showed an intrauterine foreign body that appeared implanted within the myometrium with the width of a common straw and an indeterminate length. An approximately 8-week-old live intrauterine device (IUP) was noted next to the foreign body. Upon discussing these findings with the patient, she admitted she knew she was pregnant and was trying to perform an abortion with the straw.
An obstetrics (OB) consultation was placed. The initial OB consultant stated the patient was at high risk for septic shock and miscarriage. Recommendation, prior to the consultant seeing the patient, was to admit the patient for observation and antibiotics, as well as possible dilatation and curettage if she became unstable. However, shortly after requesting the consultation, a new OB attending took over the service. The new attending stated they did not believe the patient was in any danger of infection and thought it unlikely that anything had been inserted into the uterus dismissing the ultrasound finding simply as an “artifact.” The new OB consultant’s recommendation was to discharge the patient with outpatient follow-up. Feeling uncomfortable with simply discharging a patient who was potentially at high risk for infection, the EP performed a literature search which failed to provide guidance on the management of a patient with an intrauterine foreign body that was placed post-conception and/or non-sterilely. To make matters more confusing, the patient was an African immigrant and stated she did not want her husband to know of her condition or why she was in the hospital. She listed this as one reason why she would be unable to follow-up with an outside clinic. By this time, the husband arrived at the hospital and was becoming annoyed no one would tell him about his wife’s condition. The husband’s behavior was appropriate for the (unusual) situation and the patient denied sexual, physical or emotional abuse at home. With the EP present, the patient eventually discussed the situation with her husband. Both the patient and her husband repeatedly requested removal of the foreign body due to pain, and both unequivocally stated they felt the patient’s health was more important to them than the health of the fetus. The patient was reluctant to be discharged home. At the request of the patient and her husband, the EP contacted another hospital, and the OB on call there refused to accept the patient’s transfer.
DISCUSSION
At this point, what should the EP do? This is a case that is fraught with challenges and ethical difficulty. The patient is evasive, the medicine is unusual, the consultant is obstructive, and there is potential for significant harm.
EPs always need to maintain their part of the physician-patient relationship; an EP has a duty to protect the patient from harm.1 Aside from the significant medical question of infection, there are reasons to believe the patient will be at risk of harm if she is discharged. This is a patient who has gone to unusual lengths to abort her fetus. The EP has to consider the possibility of deeper psychological problems and other self-harming behavior. Similarly, the mechanism of attempted abortion, as well as the patient’s strong desire not to let her husband know her reason for being in the hospital, strongly suggests some domestic unease. Furthermore, the patient is a foreign national who has questionable social support and will likely have less than optimal follow-up. The patient is obviously at a high risk for a bad outcome if she is discharged, and the EP should be reluctant to discharge the patient home with anything less than an optimal plan and concrete follow-up.
What makes this case more challenging than most is the medicine involved is not straightforward. Clearly, something appears to be in the uterus. Inserting foreign objects into the uterus, while not common, is certainly a known method of causing an abortion, although retaining foreign bodies is much rarer.2–4 Such foreign bodies have been known to cause infection and sepsis.5–7 Furthermore, as the numerous case reports of IUPs show, even sterile foreign bodies can lead to perforation and migration with their respective complications.8–10 However, the exact risk of infection and perforation is unknown, as is the timeline in which they may occur. At best, one can say that the patient appears to be in danger of infection with a distinct possibility of septic shock. Nonetheless, the patient had normal vital signs, appeared non-toxic, and was not in a life-threatening condition.
It is at this point one turns to consultants for clarification and guidance, as the decisions for optimal medical care are clearly outside of the EPs expertise. Unfortunately, just when a consultant was needed most, intra-specialty disagreement complicated the case. The first consultant clearly thought this case was quite serious and needed immediate action. The second consultant thought exactly the opposite downplaying the patient’s risks, questioning the patient’s credibility, denying objective evidence of the situation (the ultrasound of the straw), and making recommendations that appeared solely focused on discharging the patient.
Thankfully, situations such as this one are noteworthy for their infrequency, and the objectivity of one’s consultants is rarely called into question. However, it is a situation that EPs ought to be prepared for. One of the unique aspects of emergency medicine is that we are more at the mercies of our consultants than any other hospital service. Our consultants have specialized medical knowledge, admit all of our patients, perform vital interventions, and provide almost all of our follow-up patient care. If an irreconcilable disagreement arises between the EP and a consultant, then from both a legal and a medical perspective, the EP must do, ultimately, what they believe is best for the patient; it is our primary professional responsibility to embrace patient welfare.3-11 If the consultant adamantly refuses to admit or treat the patient, several options still remain. The EP can place the patient in an observation status in the emergency department and watch for signs of instability essentially using serial reevaluations to allow the patient’s condition to indicate its progression. This also allows more time to arrange thorough out patient follow-up or to perhaps call for another consult when a more agreeable consultant is available. It would also be quite appropriate to contact the hospital’s risk management team, ombudsman, or ethics representative, both for our own protection and for the patient’s. Throughout this process, be certain to clearly and thoroughly document any concerns, as well as the steps taken to look after the patient’s welfare and the reasoning for doing so. Avoid documentation of any disagreement with the consultant being sure to limit comments to the facts of the case, rather then focusing upon frustration or anger.
CONCLUSION
In this case, the EP followed many of the above recommendations. The OB attending refused to admit the patient, and the EP had unresolved and significant worries about discharging her home. At this point, the EP called the chairman of the OB department and, after much discussion among the EP, the chairman, and the OB attending, the OB service agreed to admit the patient for observation. The patient was observed on the OB floor for one day before signing out against medical advice. Several days later, she presented to an affiliated hospital with a surgical abdomen. Emergent laparoscopy revealed a common drinking-straw in her peritoneal cavity. The patient had a miscarriage during the postoperative period.

Figure 1. Transabdominal ultrasound image showing a foreign object within the uterus.
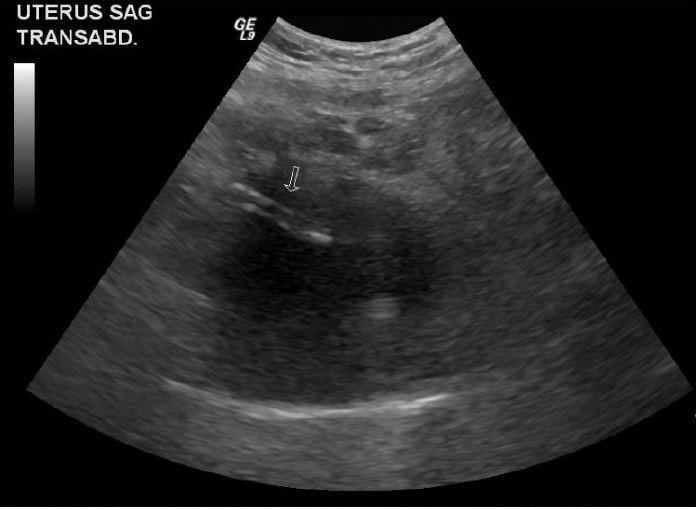
Figure 2. Transabdominal ultrasound image showing a foreign object within the uterus.

Figure 3. Transvaginal ultrasound image showing a foreign object within the uterus (arrow) next to a gestational sac.
Footnotes
Address for Correspondence: Anne Klokow, MD. Maricopa Medical Center, Department of Emergency Medicine, 2601 E. Roosevelt, Phoenix, AZ 85008. Email: amklokow@gmail.com. 3 / 2014; 15:131 – 133
Submission history: Revision received August 31, 2013; Submitted December 1, 2013; Accepted December 5, 2013
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Beauchamp TL, Childress JF. Principles of biomedical ethics; 2001.
2. Osborne DF. Attempted abortion with retention of intrauterine foreign body. Can Med Assoc J. 1964; 90(7):494-495.
3. Weisner M. Fertility and induced abortion in poor Chilean women from the perspective of medical anthropology. Enfoques Aten Prim. 1988;3(3):23-32.
4. Misago C, Fonseca W, Correia L, et al. Determinants of abortion among women admitted to hospitals in Forteleza, North Eastern Brazil. International Journal of Epidemiology. 1998;27:833-839.
5. Simetka O, Prochazka M, Huseyn Zade S, et al. Abortion induced by a foreign body with artificial perforation of the uterus, followed by sepsis, coma, necrosis of the uterus and hysterectomy. A case report. Aust N Z J Obstet Gynaecol. 2009;49(3):337-338.
6 Okonofua FE, Onwudiegwu U, Odunsi OA Illegal induced abortion: a study of 74 cases in lle-lfe, Nigeria. Trop Doc. 1992; 22:75-78.
7. Sood M, Juneja Y, Goyal U. Maternal mortality and morbidity associated with clandestine abortions. J Indian Med Assoc. 1995; 93:77-79.
8. Miranda L, Settembre A, Capasso P, et al. Laparoscopic removal of an intraperitoneal translocated intrauterine contraceptive device. Eur J Contracept Reprod Health Care. 2003;8(2):122-125.
9. Mülayim B, Mülayim S, Celik NY. A lost intrauterine device. Guess where we found it and how it happened?. Eur J Contracept Reprod Health Care. 2006;11(1):47-49.
10. Mederos R, Humaran L, Minervini D. Surgical Removal of an intrauterine device perforating the sigmoid colon: a case report. Int J Surg. 2008;6(6).
11. Code of ethics for emergency physicians. A Compendium of ACEP Policy Statements on Ethical Issues. ACEP Website. Available at: http://www.acep.org/Clinical—Practice-Magagement/Code-of-Ethicsfor-Emergency-Physicians/?_taxonomyid=117952. Last accessed
November 15, 2013.