
{kind=link}
| Author | Affiliation |
|---|---|
| Bertrand Sauneuf, MD | Medical Intensive Care Unit, Cochin Hospital, AP-HP, Paris, France |
| Benoit Champigneulle, MD | Medical Intensive Care Unit, Cochin Hospital, AP-HP, Paris, France |
| Frédéric Pène, MD, PhD | Medical Intensive Care Unit, Cochin Hospital, AP-HP, Paris, France University Paris Descartes Sorbonne Paris Cité, Paris, France |
An 80-year old man referred to the emergency department for chest pain and dyspnea on exertion reported a medical history of left pulmonary tuberculosis in babyhood, treated by therapeutic pneumothorax. This was commonly used to treat tuberculosis prior to the development of antimycobacterial agents. Successful therapeutic pneumothorax resulted in fibrosis and encapsulation of the diseased lung and containment of the infection. Forty-eight hours prior to admission, he underwent chest trauma caused by a staircase fall. Physical examination revealed extensive subcutaneous emphysema of the chest, neck and arms. Thoracic computed tomography unexpectedly revealed a single right lung expanded through the entire thorax cavity, a partial anterior pneumothorax (Figure), a fracture of the ninth right rib and extensive soft tissue emphysema. Left lung was hypoplastic in posterior position. As a consequence, mediastinum was fully shifted in left posterior position. Pneumothoraces due to trauma usually require the placement of a chest tube.1 In this case of limited anterior pneumothorax, insertion of a chest tube was not indicated, and the patient spontaneously recovered in a few days.
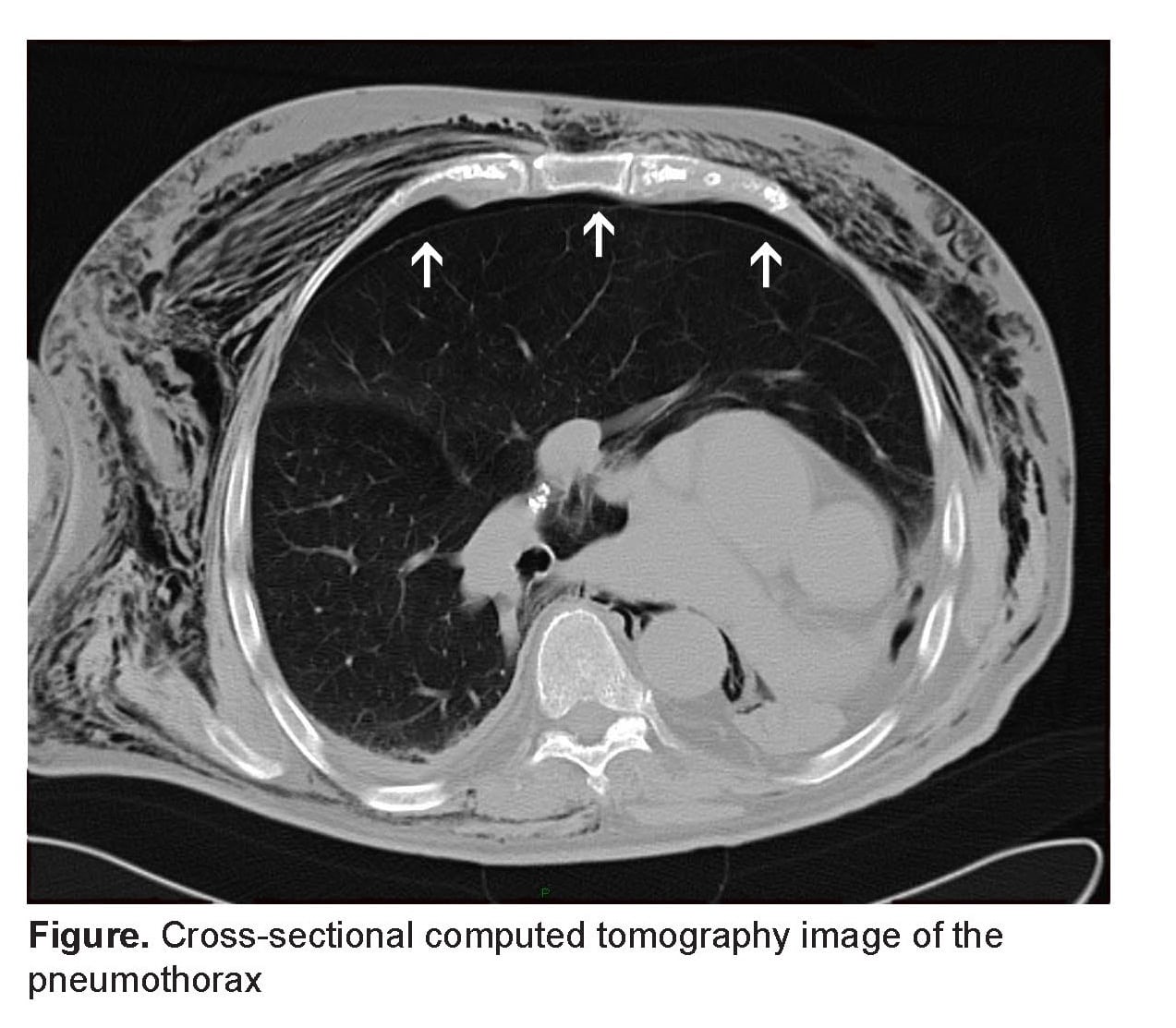
Cross-sectional computed tomography image of the pneumothorax
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted December 16, 2011; Accepted January 9, 2012
Full text available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2012.1.11602
[West J Emerg Med. 2012;13(5):444.]
Address for Correspondence: Frédéric Pene, MD, PhD, Medical Intensive Care Unit, Cochin Hospital, 27, rue du Faubourg Saint-Jacques, 75014 Paris, France
Email: frederic.pene@cch.aphp.fr
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. Haynes D, Baumann MH. Management of pneumothorax. Semin Respir Crit Care Med.2010;31:769–80. [PubMed]